The effect of autoclavable polytetrafluoroethylene strips as adjuvant to hemostatic material in periapical surgery: A technical note
December 14, 2018 / Categories: Digital Dentistry, Implant Dentistry
Cabanes Gumbau, Guillermo

Soto Peñaloza, David

Cervera Ballester, Juan

Peñarrocha Oltra, David

Peñarrocha Diago, Miguel
Abstract
Purpose
An adequate hemostasis is of utmost importance for the success of apical surgery, because it not only improves operative visibility, but also provides a dry environment within the bony crypt, ideal for an adequate retrograde obturation. This article describes a new approach for the successful management of hemostasis during apical surgery through the use of autoclavable polytetrafluoroethylene (PTFE) strips as an adjunct to epinephrine-impregnated gauze as the hemostatic material.
Materials and methods
The treatment protocol entailed the application of PTFE strips as an adjunct to epinephrine-impregnated gauze in the apical microsurgery approach, using mineral trioxide aggregate as retrograde obturation material and advanced platelet-rich fibrin plus (A-PRF+) membranes as filling material of the bony crypt.
Results
Asynergistic effect of the application of PTFE strips adjunct to epinephrine- impregnated gauze was found, yielding good intraoperative visualization and hemostasis. PTFE strips work as a mechanical barrier, and the material is easily adapted to the bony crypt size and feature by compression. Moreover, PTFE strips are easy to remove without leaving residues that may impair healing.
Conclusion
PTFE strips and epinephrine-impregnated gauze demonstrated a good synergistic effect on hemostasis. PTFE strips are a simple, innocuous and cheap means of enhancing bleeding control during apical surgery.
Keywords
Apical surgery; PTFE; hemostatic agent; oral surgery; advanced plateletrich fibrin plus.
Introduction
The use of an adequate hemostatic agent is considered of utmost importance among factors related to clinical success in apical surgery. Bleeding control improves vision at the surgical site, reducing operating time, and preventing hemorrhage and postoperative swelling.1Witherspoon DE, Gutmann JL. Haemostasis in periradicular surgery. → Int Endod J. 1996 May;29(3):135–49. Different techniques and materials have been used to control hemostasis in apical surgery, the most used being bone wax, collagen membranes, ferric sulfate, epinephrine and aluminum chloride.
Kim and Rethnam in 1997 described that a good hemostatic agent should stop the hemorrhage in a short period, be easy to handle, be biocompatible, be relatively cheap and secure, and not complicate or delay the wound healing.2Kim S, Rethnam S. Hemostasis in endodontic microsurgery. → Dent Clin North Am. 1997 Jul;41(3):499–511. An optimal surgical dry environment is necessary to achieve the best results regarding material properties during retrograde obturation (e.g., MTA, Biodentine and super EBA). Nowadays, the search for an ideal hemostatic agent continues, and different agents (e.g., calcium sulphate, ferric sulphate, collagen plus epinephrine, and aluminum chloride-based paste Expasyl) have been tested and documented in clinical studies.3Clé-Ovejero A, Valmaseda-Castellón E. Haemostatic agents in apical surgery. A systematic review. → Med Oral Patol Oral Cir Bucal. 2016 Sep;21(5):e652–7. doi:10.4317/medoral.21109.
A recent adequate sample size clinical trial demonstrated the superiority in terms of bleeding control of aluminum chloride-based paste Expasyl over a gauze impregnated with epinephrine, but without statistically significant differences. Nevertheless, to date, there is no consensus about which of them is the best option.4Witherspoon DE, Gutmann JL. Haemostasis in periradicular surgery. → Int Endod J. 1996 May;29(3):135–49. Moreover, translational evidence suggests that Expasyl plus ferric sulphate or electrocauterization are superior regarding bleeding control compared with other hemostatic agents in rabbit calvaria.5Jensen SS, Yazdi PM, Hjørting-Hansen E, Bosshardt DD, Von Arx T. Haemostatic effect and tissue reactions of methods and agents used for haemorrhage control in apical surgery. → Int Endod J. 2010 Jan;43(1):57–63. doi:10.1111/j.1365-2591.2009.01637.x. However, they were accompanied by unfavorable tissue reactions, such as necrotic bone, presence of inflammatory cells and absence of bone repair.6Jensen SS, Yazdi PM, Hjørting-Hansen E, Bosshardt DD, Von Arx T. Haemostatic effect and tissue reactions of methods and agents used for haemorrhage control in apical surgery. → Int Endod J. 2010 Jan;43(1):57–63. doi:10.1111/j.1365-2591.2009.01637.x. To reduce these effects, it has been suggested that bone defects should be freshened with a rotary instrument before suturing.
Several hemostatic agents are liquids (e.g., epinephrine and ferric sulphate) and carriers are used for their delivery (e.g., resorbable collagen sponges and cotton pellets).7Jang Y, Kim H, Roh BD, Kim E. Biologic response of local hemostatic agents used in endodontic microsurgery. → Restor Dent Endod. 2014 May;39(2):79–88. doi:10.5395/ rde.2014.39.2.79. The ideal carrier material should be able to be removed without leaving traces that impair healing.
Polytetrafluoroethylene (PTFE) or plumber’s tape is used for multiple applications in dentistry because it is a nonstick, inert and pliable material.8Sattar MM, Patel M, Alani A. Clinical applications of polytetrafluoroethylene (PTFE) tape in restorative dentistry. → Br Dent J. 2017 Feb;222(3):151–8. doi:10.1038/sj.bdj.2017.110. In dental implant-supported prosthodontics, it is used like a sealer material for implant abutment screw holes,9Alshehri M, Albaqiah H. Antimicrobial efficacy of materials used for sealing the implant abutment screw hole: an in vitro evaluation. → Implant Dent. 2017 Dec;26(6):911–4. doi:10.1097/ ID.0000000000000688. minimizing the risk of screw head damage during retrieval procedures.10Sattar MM, Patel M, Alani A. Clinical applications of polytetrafluoroethylene (PTFE) tape in restorative dentistry. → Br Dent J. 2017 Feb;222(3):151–8. doi:10.1038/sj.bdj.2017.110. PTFE is nonfilamentous and thus easier to remove compared with cotton pellets, which tear easily during removal. PTFE tape is also used as a spacer beneath temporary restorative obturation material in root canal therapy, yielding less bacterial leakage.11Prabhakar AR, Dixit K, Raju O. Microbiologic evaluation of cotton and polytetrafluoroethylene (PTFE) tape as endodontic spacer materials in primary molars an in vivo study. → J Clin Pediatr Dent. 2018;42(1):21–6. doi:10.17796/1053- 4628-42.1.4.
PTFE strips can be compacted against the walls of the bony crypt after ostectomy. The material can be adapted to the defect size and through compression works as a mechanical hemostatic barrier. Hence, the present article was aimed at introducing a novel approach to managing the bleeding during periapical surgery, through the use of PTFE strips as a mechanical hemostatic material adjunct to epinephrineimpregnated gauze.

Fig. 1
Intraoral view. Maxillary anterior region without swelling or pathological signs.

Fig. 2
Periapical radiograph of the anterior incisors that had undergone root canal therapy. Apical radiolucencies can be observed surrounding the root apices.
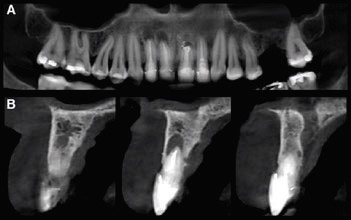
Fig. 3
CBCT images. (A) Panoramic view of the maxilla, where apical lesions can be more clearly seen around the incisal apices. (B) The CBCT sagittal slice confirmed that the apical defects were related to the root canal retreatment.
Technical report and clinical case
A brief description of the periapical surgery technique is first given to depict the use of PTFE strips as an adjunct for establishing hemostasis, based on a clinical case and its postoperative care. The case is detailed thereafter.
Materials and methods
The surgery was carried out under local anesthesia with 4% articaine and 1:100,000 epinephrine (Inibsa). The flap approach entailed making a paramarginal incision. Once the flap had been elevated, the inflammatory tissue surrounding the root apex, forming a bone crypt, was debrided using manual curettes. Hemostasis was achieved using epinephrine-impregnated gauze, subsequently reinforced with PTFE strips previously sterilized by autoclave, and compacted using an amalgam ball burnisher-plugger within the bony crypt surrounding the tooth apex. The root ends were inspected using a rigid endoscope (Möller-Wedel). The root-end cavities were prepared with sonic-driven microtips and ultrasonic tips (Piezon Master 400, EMS Electro Medical Systems), and then were retrofilled with mineral trioxide aggregate (MTA; Dentsply Tulsa Dental Specialties). Finally, the quality of the retrograde fillings was inspected using a rigid endoscope (Möller-Wedel).
The bony crypts were regenerated using an autologous platelet concentrate. Membranes of advanced platelet-rich fibrin plus (A-PRF+; Process for PRF, Nice, France) were prepared from the patient’s venous blood, collected in 3 × 10 mL sterile glass vacuum tubes (plain vacuum tube A-PRF™+; Process for PRF, Nice, France) and centrifuged at 1,300 rpm × 8 min (200 × g). This process allows one to obtain a 3-D fibrin mesh enriched with platelets, and growth factor released from platelet alpha granules after a slow activation without additives. This mean of production provides a source of biological signals and growth factors that enhances wound repair and angiogenesis.12Ghanaati S, Booms P, Orlowska A, Kubesch A, Lorenz J, Rutkowski J, Landes C, Sader R, Kirkpatrick C, Choukroun J. Advanced platelet-rich fibrin: a new concept for cell-based tissue engineering by means of inflammatory cells. → J Oral Implantol. 2014 Dec;40(6):679–89. doi:10.1563/ aaid-joi-D-14-00138.,13El Bagdadi K, Kubesch A, Yu X, Al-Maawi S, Orlowska A, Dias A, Booms P, Dohle E, Sader R, Kirkpatrick CJ, Choukroun J, Ghanaati S. Reduction of relative centrifugal forces increases growth factor release within solid platelet- rich-fibrin (PRF)-based matrices: a proof of concept of LSCC (low speed centrifugation concept). → Eur J Trauma Emerg Surg. 2017 Mar 21:1–13. doi:10.1007/s00068-017-0785-7. [Epub ahead of print].,14Dohan Ehrenfest DM, Del Corso M, Diss A, Mouhyi J, Charrier JB. Three- dimensional architecture and cell composition of a Choukroun’s platelet-rich fibrin clot and membrane. → J Periodontol. 2010 Apr;81(4):546–55. doi:10.1902/jop.2009.090531.
Clinical case
A 57-year-old female patient was referred to our clinic because of an asymptomatic apical lesion involving single-rooted teeth in the anterior maxilla. The patient reported no relevant systemic condition or allergies. The clinical exploration found good oral hygiene and periodontal status. The patient reported that she smoked 11–15 cigarettes per day, and no softtissue alterations in the region of interest were observed (Fig. 1). In an intraoral radiograph, the 2 central incisors and 1 lateral incisor that had undergone root canal therapy showed apical radiolucencies surrounding the root apices. One central incisor showed a previous periapical surgery (Fig. 2). The CBCT study confirmed that not only the central but also the contiguous lateral and central incisors were affected, as verified in the panoramic view and sagittal slices (Fig. 3). No pathological periodontal pockets were present but a slight gingival recession in the buccal side was present, of type I according to Miller.15Miller PD. A classification of marginal tissue recession. → Int J Periodontics Restorative Dent. 1985;5(2):8–13.
A paramarginal incision was performed to reach the affected area, and a full-thickness surgical flap was raised at the buccal side, followed by ostectomy and apicoectomy (Fig. 4). Hemostasis was then performed using epinephrineimpregnated gauze and PTFE strips, and the retrograde cavity was prepared and sealed with MTA (Fig. 5). Excess material was removed with manual curettes and rotary instruments (Fig. 6). The root integrity and apical filling were ascertained using a rigid endoscope (Fig. 7).
The bony defects of the affected apical areas were filled with pieces of A-PRF+ membranes (Fig. 8). After cleaning the intervention area with saline solution, primary wound closure was accomplished with multiple interrupted sutures (Fig. 9). A postoperative periapical radiograph was taken (Fig. 10).
-

-
Fig. 4
Buccal lesions were accessed through a paramarginal flap. The apical lesions were accessed after osteotomy and granulation tissue debridement.
-

-
Fig. 5
Bony crypt bleeding was controlled by applying epinephrine-impregnated gauze and PTFE strips packaged with pressure against the bony walls. The cavity preparation was done using an ultrasonic tip, then MTA filling material was used to obturate the retrograde cavity. Good bleeding control can be observed.
-

-
Fig. 6
MTA excess was removed using a surgical curette.
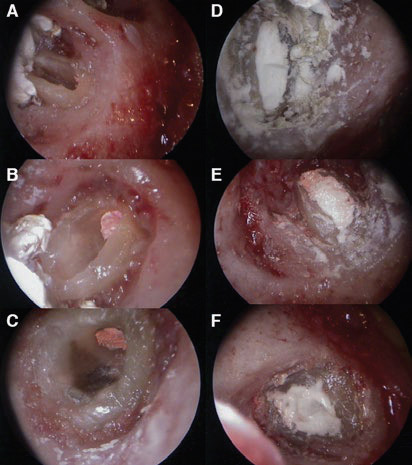
Rigid endoscopic images. Apical preparation and root canal integrity were ascertained.
(A–C) Retrograde obturation quality was inspected.
(D–F) The good bleeding control can be appreciated.
-

-
Fig. 8A
Before flap repositioning, the bony crypt was filled with pieces of autologous fibrin matrix, A-PRF+ membrane.
-

-
Fig. 8B
A-PRF+ membranes were placed inside the apical bony crypts.

Fig. 9
Flap suturing with resorbable material.

Fig. 10
Postoperative periapical radiograph.
Postoperative care
The patient was prescribed amoxicillin (500 mg/8 h) for 5 days after the intervention, ibuprofen (400 mg/8 h) for 4 days, a 0.12% chlorhexidine rinse (twice a day) for 7 days, and paracetamol (500 mg on demand) in the event of intense pain. The sutures were removed after 1 week.
Discussion
Achieving success in apical surgery requires adequate bleeding control to reduce the surgery time, enhance operative vision and diminish postoperative complications such as swelling and patient discomfort. Most importantly, it allows us to guarantee optimal conditions for the setting of the retrograde sealing material.
Hemostatic agents and materials by definition are classified according to their properties. They can be chemical or mechanical, working as a barrier, such as bone wax. Bone wax has been used for many years and is easy to handle, though remaining traces of this material can cause adverse tissue reactions.16Sauveur G, Roth F, Sobel M, Boucher Y. The control of haemorrhage at the operative site during periradicular surgery. → Int Endod J. 1999 May;32(3):225–8. Similar problems have been observed with ferric sulfate: When not completely eliminated from the surgical site, it gives rise to foreign-body reactions that complicate healing.17Lemon RR, Steele PJ, Jeansonne BG. Ferric sulfate hemostasis: effect on osseous wound healing. Left in situ for maximum exposure. → J Endod. 1993 Apr;19(4):170–3.
The hemostatic efficacy and the tissue reactions of bone wax, ferric sulfate, aluminum chloride, and a combination of aluminum chloride and ferric sulfate were assessed previously by an experimental report.18von Arx T, Jensen SS, Hänni S, Schenk RK. Haemostatic agents used in periradicular surgery: an experimental study of their efficacy and tissue reactions. → Int Endod J. 2006 Oct;39(10):800–8. doi:10.1111/j.1365-2591.2006.01152.x. The authors indicated that Expasyl alone or in combination with ferric sulfate was the most effective agent.19von Arx T, Jensen SS, Hänni S, Schenk RK. Haemostatic agents used in periradicular surgery: an experimental study of their efficacy and tissue reactions. → Int Endod J. 2006 Oct;39(10):800–8. doi:10.1111/j.1365-2591.2006.01152.x. Another study compared 5 hemostatic techniques following the same preclinical design reported by von Arx et al. in 2006 and found that the most effective methods for reducing bleeding were Expasyl + Stasis and electrocautery.20von Arx T, Jensen SS, Hänni S, Schenk RK. Haemostatic agents used in periradicular surgery: an experimental study of their efficacy and tissue reactions. → Int Endod J. 2006 Oct;39(10):800–8. doi:10.1111/j.1365-2591.2006.01152.x. However, this bleeding control efficacy was accompanied by unfavorable tissue reactions, such as necrotic bone, inflammatory cells and the absence of bone repair.21Jensen SS, Yazdi PM, Hjørting-Hansen E, Bosshardt DD, Von Arx T. Haemostatic effect and tissue reactions of methods and agents used for haemorrhage control in apical surgery. → Int Endod J. 2010 Jan;43(1):57–63. doi:10.1111/j.1365-2591.2009.01637.x. Using impregnated gauze with epinephrine showed good hemostatic results, but inferior to those obtained with Expasyl.22Menéndez-Nieto I, Cervera-Ballester J, Maestre-Ferrín L, Blaya-Tárraga JA, Peñarrocha-Oltra D, Peñarrocha-Diago M. Hemostatic agents in periapical surgery: a randomized study of gauze impregnated in epinephrine versus aluminum chloride. → J Endod. 2016 Nov;42(11):1583–7. doi:10.1016/j. joen.2016.08.005. The advantage of this method is that it does not leave residues that might affect wound healing after apical surgery.
Available evidence is not conclusive regarding the best hemostatic agent, but denotes that being cheap and easy to handle are among the desirable characteristics.23Kim S, Rethnam S. Hemostasis in endodontic microsurgery. → Dent Clin North Am. 1997 Jul;41(3):499–511. PTFE tape is cheap, easy to handle and to remove from the bony crypt, leaving no residues, and autoclavable. For the above-mentioned reasons, we tested sterilized PTFE strips as a new means of enhancing the already good bleeding control usually achieved with epinephrine- impregnated gauze.
The use of PTFE strips combined with epinephrine- impregnated gauze might provide bleeding control comparable to that of Expasyl without the drawbacks of this method, difficulty of removal and risk of postoperative tissue reactions.
Conclusion
PTFE strips and epinephrine-impregnated gauze demonstrated a good synergistic effect on hemostasis. PTFE strips are a simple, innocuous and cheap means of enhancing bleeding control during apical surgery. Clinical studies should be done to evaluate this technique.

Interview
with Guillermo Cabanes Gumbau
Why did you conduct the research reported on in this paper?
For what reasons could others cite your paper?
3. How could your study’s findings have an impact on dentistry? And what is the relevance of your study’s findings to the daily practice of a dentist?
What are your recommendations for further investigation of the topic of your article?
References
| 1, 4. | ↑ | Witherspoon DE, Gutmann JL. Haemostasis in periradicular surgery. → Int Endod J. 1996 May;29(3):135–49. |
| 2, 23. | ↑ | Kim S, Rethnam S. Hemostasis in endodontic microsurgery. → Dent Clin North Am. 1997 Jul;41(3):499–511. |
| 3. | ↑ | Clé-Ovejero A, Valmaseda-Castellón E. Haemostatic agents in apical surgery. A systematic review. → Med Oral Patol Oral Cir Bucal. 2016 Sep;21(5):e652–7. doi:10.4317/medoral.21109. |
| 5, 6, 21. | ↑ | Jensen SS, Yazdi PM, Hjørting-Hansen E, Bosshardt DD, Von Arx T. Haemostatic effect and tissue reactions of methods and agents used for haemorrhage control in apical surgery. → Int Endod J. 2010 Jan;43(1):57–63. doi:10.1111/j.1365-2591.2009.01637.x. |
| 7. | ↑ | Jang Y, Kim H, Roh BD, Kim E. Biologic response of local hemostatic agents used in endodontic microsurgery. → Restor Dent Endod. 2014 May;39(2):79–88. doi:10.5395/ rde.2014.39.2.79. |
| 8, 10. | ↑ | Sattar MM, Patel M, Alani A. Clinical applications of polytetrafluoroethylene (PTFE) tape in restorative dentistry. → Br Dent J. 2017 Feb;222(3):151–8. doi:10.1038/sj.bdj.2017.110. |
| 9. | ↑ | Alshehri M, Albaqiah H. Antimicrobial efficacy of materials used for sealing the implant abutment screw hole: an in vitro evaluation. → Implant Dent. 2017 Dec;26(6):911–4. doi:10.1097/ ID.0000000000000688. |
| 11. | ↑ | Prabhakar AR, Dixit K, Raju O. Microbiologic evaluation of cotton and polytetrafluoroethylene (PTFE) tape as endodontic spacer materials in primary molars an in vivo study. → J Clin Pediatr Dent. 2018;42(1):21–6. doi:10.17796/1053- 4628-42.1.4. |
| 12. | ↑ | Ghanaati S, Booms P, Orlowska A, Kubesch A, Lorenz J, Rutkowski J, Landes C, Sader R, Kirkpatrick C, Choukroun J. Advanced platelet-rich fibrin: a new concept for cell-based tissue engineering by means of inflammatory cells. → J Oral Implantol. 2014 Dec;40(6):679–89. doi:10.1563/ aaid-joi-D-14-00138. |
| 13. | ↑ | El Bagdadi K, Kubesch A, Yu X, Al-Maawi S, Orlowska A, Dias A, Booms P, Dohle E, Sader R, Kirkpatrick CJ, Choukroun J, Ghanaati S. Reduction of relative centrifugal forces increases growth factor release within solid platelet- rich-fibrin (PRF)-based matrices: a proof of concept of LSCC (low speed centrifugation concept). → Eur J Trauma Emerg Surg. 2017 Mar 21:1–13. doi:10.1007/s00068-017-0785-7. [Epub ahead of print]. |
| 14. | ↑ | Dohan Ehrenfest DM, Del Corso M, Diss A, Mouhyi J, Charrier JB. Three- dimensional architecture and cell composition of a Choukroun’s platelet-rich fibrin clot and membrane. → J Periodontol. 2010 Apr;81(4):546–55. doi:10.1902/jop.2009.090531. |
| 15. | ↑ | Miller PD. A classification of marginal tissue recession. → Int J Periodontics Restorative Dent. 1985;5(2):8–13. |
| 16. | ↑ | Sauveur G, Roth F, Sobel M, Boucher Y. The control of haemorrhage at the operative site during periradicular surgery. → Int Endod J. 1999 May;32(3):225–8. |
| 17. | ↑ | Lemon RR, Steele PJ, Jeansonne BG. Ferric sulfate hemostasis: effect on osseous wound healing. Left in situ for maximum exposure. → J Endod. 1993 Apr;19(4):170–3. |
| 18, 19, 20. | ↑ | von Arx T, Jensen SS, Hänni S, Schenk RK. Haemostatic agents used in periradicular surgery: an experimental study of their efficacy and tissue reactions. → Int Endod J. 2006 Oct;39(10):800–8. doi:10.1111/j.1365-2591.2006.01152.x. |
| 22. | ↑ | Menéndez-Nieto I, Cervera-Ballester J, Maestre-Ferrín L, Blaya-Tárraga JA, Peñarrocha-Oltra D, Peñarrocha-Diago M. Hemostatic agents in periapical surgery: a randomized study of gauze impregnated in epinephrine versus aluminum chloride. → J Endod. 2016 Nov;42(11):1583–7. doi:10.1016/j. joen.2016.08.005. |





Leave a Reply
Be the First to Comment!