The relationship between oral squamous cell carcinoma and dental implants: A literature review
December 14, 2018 / Categories: Digital Dentistry, Implant Dentistry

Rodríguez Caballero, Ángela

Romero Ruiz, Manuel María

Serrera Figallo, María Angeles

Gutiérrez Pérez, José Luis

Torres Lagares, Daniel
Abstract
Purpose
The aim of this article is to provide a thorough review of the possible relationship between dental implants and the incidence of oral cancer, particularly emphasizing the clinical data, to allow an early diagnosis of cancer and avoid mistakes in diagnosing cancer or regular periimplant inflammatory conditions.
Materials and methods
A literature search on Medline/PubMed was performed. The criteria for consideration were articles published between 1999 and 2017, with the following MeSH terms: “oral squamous cell carcinoma,” “dental implants,” “osseointegrated,” and “periimplant tumor.” To be considered, they had to be
1. original studies;
2. clinical trials, meta-analyses, randomized controlled trials, or reviews;
3. on oral squamous cell carcinoma developed around osseointegrated implants;
4. papers published in English; and
5. studies done in humans.
The papers were selected by the authors of this study and validated by agreement.
Results
Initially, 143 papers were selected, of which only 12 were kept after excluding those not matching the inclusion criteria. An average of 2 implants were present in patients between 42 and 80 years old. Regarding the location of the tumors, 88.23% were located in the lower jaw, mainly (76.46%) in the posterior area. Only 2 out of the 17 (11.77%) were located on the edge of the tongue.
Conclusion
An appropriate preoperative study should be done on patients at risk, and the prosthesis should be designed to allow easy removal for tissue examination. A histopathological test should be performed in the case of inflammatory tissue in the periimplant area.
Keywords
Oral cancer; dental implants; relationship.
Introduction
Oral cancer represents 2% of all malignant tumors. Approximately 90% of oral carcinoma is squamous cell carcinoma of the oral epithelium (OSCC) of the oral epithelium, while the other 10% is tumors of other histological origin, being extremely rare malign odontogenic tumors and metastatic tumors from carcinomas located at distance.1Ferlay J, Shin HR, Bray F, Formah D, Mathers C, Parkin DM. Estimates of worldwide burden of cancer in 2008: GLOBOCAN 2008. → Int J Cancer. 2010 Dec 15;127(12):2893–917. Only 1% of oral carcinoma cases develop metastasis, although metastases in the hard tissue of the maxillofacial area are more common compared with those in the soft tissue (2:1 relation).2Ferlay J, Shin HR, Bray F, Formah D, Mathers C, Parkin DM. Estimates of worldwide burden of cancer in 2008: GLOBOCAN 2008. → Int J Cancer. 2010 Dec 15;127(12):2893–917.,3Johnson NW, Jayasekara P, Amarasinghe AA. Squamous cell carcinoma and precursor lesions of the oral cavity: epidemiology and aetiology. → Periodontol 2000. 2011 Oct;57(1):19–37. The etiology of OSCC is multifactorial. Oral hygiene and toxic habits such as alcohol- and tobacco-related factors have been proven to be involved.4Johnson NW, Jayasekara P, Amarasinghe AA. Squamous cell carcinoma and precursor lesions of the oral cavity: epidemiology and aetiology. → Periodontol 2000. 2011 Oct;57(1):19–37.,5Rothenberg SM, Ellisen LW. The molecular pathogenesis of head and neck squamous cell carcinoma. → J Clin Invest. 2012 Jun;122(6):1951–7.,6Hirota SK, Braga FP, Penha SS, Sugaya NN, Migliari DA. Risk factors for oral squamous cell carcinoma in young and older Brazilian patients: a comparative analysis. → Med Oral Patol Oral Cir Bucal. 2008 Apr;13(4):E227–31. The risk of malignancy is increased in the presence of oral lesions like leukoplakia or erythroplakia, lichen planus or human papillomavirus lesions. Patients with a previous history of carcinoma also have a greater risk of developing a second primary neoplasm.7Hirota SK, Braga FP, Penha SS, Sugaya NN, Migliari DA. Risk factors for oral squamous cell carcinoma in young and older Brazilian patients: a comparative analysis. → Med Oral Patol Oral Cir Bucal. 2008 Apr;13(4):E227–31.,8Liang C, Marsit CJ, McClean MD, Nelson HH, Christensen BC, Haddad RI, Clark JR, Wein RO, Grillone GA, Houseman EA, Halec G, Waterboer T, Pawlita M, Krane JF, Kelsey KT. Biomarkers of HPV in head and neck squamous cell carcinoma. → Cancer Res. 2012 Oct;72(19):5004–13.
Implant placement for the oral rehabilitation of the partially or completely edentulous patient is nowadays a predictable treatment option and allows recovery of the loss of esthetics and function.9Buser D, Janner SF, Wittneben JG, Brägger U, Ramseier CA, Salvi GE. 10-year survival and success rates of 511 titanium implants with a sandblasted and acid-etched surface: a retrospective study in 303 partially edentulous patients. → Clin Implant Dent Relat Res. 2012 Dec;14(6):839–51.,10Jiang BQ, Lan J, Huang HY, Liang J, Ma XN, Huo LD, Xu X. A clinical study on the effectiveness of implant supported dental restoration in patients with chronic periodontal diseases. → Int J Oral Maxillofac Surg. 2013 Feb;42(2):256–9. doi:10.1016/j. ijom.2012.08.001. Epub 2012 Sep 26. Long-term success rates have been reported, even in patients particularly difficult to treat. However, there is no lack of complications that may occur, and among the most common is a chronic inflammatory process of both soft and hard tissue, separately or at the same time.11Javed F, Al-Hezaimi K, Al-Rasheed A, Almas K, Romanos GE. Implant survival rate after oral cancer therapy: a review. → Oral Oncol. 2010 Dec;46(12):854–9.,12Bianchi B, Ferri A, Ferrari S, Leporati M, Copelli C, Ferri T, Sesenna E. Mandibular resection and reconstruction in the management of extensive ameloblastoma. → J Oral Maxillofac Surg. 2013 Mar;71(3):528–37. doi:10.1016/j. joms.2012.07.004. Epub 2012 Sep 27.,13Jacobsen C, Kruse A, Lübbers HT, Zwahlen R, Studer S, Zemann W, Seifert B, Grätz KW. Is mandibular reconstruction using vascularized fibula flaps and dental implants a reasonable treatment? → Clin Implant Dent Relat Res. 2014 Jun;16(3):419–28. doi:10.1111/ cid.12004. Epub 2012 Sep 21.,14Anne-Gaëlle B, Samuel S, Julie B, Renaud L, Pierre B. Dental implant placement after mandibular reconstruction by microvascular free fibula flap: current knowledge and remaining questions. → Oral Oncol. 2011 Dec;47(12):1099–104.,15Carbiner R, Jerjes W, Shakib K, Giannoudis PV, Hopper C. Analysis of the compatibility of dental implant systems in fibula free flap reconstruction. → Head Neck Oncol. 2012 Jun 21;4:37.
At the 2008 European Workshop on Periodontology, 2 possibilities of diagnosis were defined: periimplant mucositis and periimplantitis. 16Lindhe J, Meyle J; Group D of European Workshop on Periodontology. Peri-implant diseases: consensus report of the Sixth European Workshop on Periodontology. → J Clin Periodontol. 2008 Sep;35(8 Suppl):282–5. The former describes an inflammatory lesion located on the mucosa that is clinically reddened (erythematosus) and bleeds on probing, although with no bone loss. For periimplantitis, however, there is bone loss in addition to the other signs and symptoms, and it is commonly associated with suppuration and deep pockets. Periimplantitis and periimplant mucositis occur in up to 80% of patients and affect up to 50% of implants. Risk factors for periimplantitis are poor oral hygiene, a history of periodontitis, diabetes mellitus, tobacco use, alcohol use and genetic predisposition. Of all these risk factors, only poor oral hygiene and tobacco use have the best scientific evidence to support their connection to periimplantitis, the rest of the risk factors being insufficiently proven.17Lindhe J, Meyle J; Group D of European Workshop on Periodontology. Peri-implant diseases: consensus report of the Sixth European Workshop on Periodontology. → J Clin Periodontol. 2008 Sep;35(8 Suppl):282–5.
There are few published cases on osseointegrated dental implants associated with OSCC; however, there is scientific evidence to support that, in some cases, OSCC surrounding dental implants has a very similar appearance to that of periimplantitis, with mucosal reddening and bone loss.
The aim of this research is to perform a thorough review of the relationship between OSCC and dental implants, trying at the same time to identify the various clinical presentations and the eventual risk factors. It is also intended to identify at an early stage those clinical elements that can lead to OSCC, facilitating biopsy and early diagnosis.
Materials and methods
A search on Medline/PubMed was carried out on the relationship between dental implants and OSCC. Regarding the search strategy, papers published between June 1999 and March 2017, including these dates, were included. The MeSH resource was used, selecting as search terms “oral squamous cell carcinoma,” “dental implants,” “osseointegrated,” and “periimplant tumor.” The criteria for selection were
- 1. original studies;
- clinical trials, meta-analyses, randomized controlled trials, or literature reviews;
- OSCC developed around dental implants;
- articles published in English;
- articles of studies in humans.
The articles were selected by the researchers based on their titles and abstracts and validated by consensus.”. All those articles related to OSCC in relation to dental implants (clinical cases with histopathological tests). Those articles where the patient’s age, tumor location or type was not specified were excluded.
Results
Initially, 143 articles were selected, of which 132 did not meet all of the inclusion criteria and therefore were excluded. In total, 12 articles were selected18Block MS, Scheufler E. Squamous cell carcinoma appearing as peri-implant bone loss: a case report. → J Oral Maxillofac Surg. 2001 Nov;59(11):1349–52.,19Czerninski R, Kaplan I, Almoznino G, Maly A, Regev E. Oral squamous cell carcinoma around dental implants. → Quintessence Int. 2006 Oct;37(9):707–11.,20Eguia del Valle A, Martínez-Conde Llamosas R, López Vicente J, Uribarri Etxebarria A, Aguirre Urizar JM. Primary oral squamous cell carcinoma arising around dental osseointegrated implants mimicking peri-implantitis. → Med Oral Patol Oral Cir Bucal. 2008 Aug 1;13(8):E489–91.,21Kwok J, Eyeson J, Thompson I, McGurk M. Dental implants and squamous cell carcinoma in the at risk patient—report of three cases. → Br Dent J. 2008 Nov;205(10):543–5.,22Gallego L, Junquera L, Llorente S. Oral carcinoma associated with implant- supported overdenture trauma: a case report. → Dent Traumatol. 2009 Feb;25(1):e3–4.,23Gulati A, Puthussery FJ, Downie IP, Flood TR. Squamous cell carcinoma presenting as peri-implantitis: a case report. → Ann R Coll Surg Engl. 2009 Oct;91(7):W8–10.,24De Ceulaer J, Magremanne M, van Veen A, Scheerlinck J. Squamous cell carcinoma recurrence around dental implants. → J Oral Maxillofac Surg. 2010 Oct;68(10):2507–12.,25Meijer GJ, Dieleman FJ, Bergé SJ, Merkx MA. Removal of an oral squamous cell carcinoma including parts of osseointegrated implants in the marginal mandibulectomy. A case report. → Oral Maxillofac Surg. 2010 Dec;14(4):253–6.,26Agostini T, Sacco R, Bertolai R, Acocella A, Colafranceschi M, Lazzeri D. Peri-implant squamous odontogenic tumor. → J Craniofac Surg. 2011 May;22(3):1151–7. 23. Jané-Salas E, López-López J, Roselló- Llabrés X, Rodríguez-Argueta OF, Chimenos-Küstner E. Relationship between oral cancer and implants: clinical cases and systematic literature review. → Med Oral Patol Oral Cir Bucal. 2012 Jan 1;17(1):e23–8.,27Jané-Salas E, López-López J, Roselló- Llabrés X, Rodríguez-Argueta OF, Chimenos-Küstner E. Relationship between oral cancer and implants: clinical cases and systematic literature review. → Med Oral Patol Oral Cir Bucal. 2012 Jan 1;17(1):e23–8.,28Pfammatter C, Lindenmüller IH, Lugli A, Filippi A, Kühl S. Metastases and primary tumors around dental implants: a literature review and case report of peri-implant pulmonary metastasis. → Quintessence Int. 2012 Jul–Aug;43(7):563–70.,29Javed F, Al-Askar M, Qayyum F, Wang HL, Al-Hezaimi K. Oral squamous cell carcinoma arising around osseointegrated dental implants. → Implant Dent. 2012 Aug;21(4):280–6. and processed for collection of data. They were 4 literature reviews, involving 5 clinical cases;30Czerninski R, Kaplan I, Almoznino G, Maly A, Regev E. Oral squamous cell carcinoma around dental implants. → Quintessence Int. 2006 Oct;37(9):707–11.,31Jané-Salas E, López-López J, Roselló- Llabrés X, Rodríguez-Argueta OF, Chimenos-Küstner E. Relationship between oral cancer and implants: clinical cases and systematic literature review. → Med Oral Patol Oral Cir Bucal. 2012 Jan 1;17(1):e23–8.,32Pfammatter C, Lindenmüller IH, Lugli A, Filippi A, Kühl S. Metastases and primary tumors around dental implants: a literature review and case report of peri-implant pulmonary metastasis. → Quintessence Int. 2012 Jul–Aug;43(7):563–70.,33Javed F, Al-Askar M, Qayyum F, Wang HL, Al-Hezaimi K. Oral squamous cell carcinoma arising around osseointegrated dental implants. → Implant Dent. 2012 Aug;21(4):280–6. 1 longitudinal randomized case–control trial;34De Ceulaer J, Magremanne M, van Veen A, Scheerlinck J. Squamous cell carcinoma recurrence around dental implants. → J Oral Maxillofac Surg. 2010 Oct;68(10):2507–12. 1 case series;35Kwok J, Eyeson J, Thompson I, McGurk M. Dental implants and squamous cell carcinoma in the at risk patient—report of three cases. → Br Dent J. 2008 Nov;205(10):543–5. and 6 welldocumented case reports.36Block MS, Scheufler E. Squamous cell carcinoma appearing as peri-implant bone loss: a case report. → J Oral Maxillofac Surg. 2001 Nov;59(11):1349–52.,37Eguia del Valle A, Martínez-Conde Llamosas R, López Vicente J, Uribarri Etxebarria A, Aguirre Urizar JM. Primary oral squamous cell carcinoma arising around dental osseointegrated implants mimicking peri-implantitis. → Med Oral Patol Oral Cir Bucal. 2008 Aug 1;13(8):E489–91.,38Gallego L, Junquera L, Llorente S. Oral carcinoma associated with implant- supported overdenture trauma: a case report. → Dent Traumatol. 2009 Feb;25(1):e3–4.,39Gulati A, Puthussery FJ, Downie IP, Flood TR. Squamous cell carcinoma presenting as peri-implantitis: a case report. → Ann R Coll Surg Engl. 2009 Oct;91(7):W8–10.,40Meijer GJ, Dieleman FJ, Bergé SJ, Merkx MA. Removal of an oral squamous cell carcinoma including parts of osseointegrated implants in the marginal mandibulectomy. A case report. → Oral Maxillofac Surg. 2010 Dec;14(4):253–6.,41Agostini T, Sacco R, Bertolai R, Acocella A, Colafranceschi M, Lazzeri D. Peri-implant squamous odontogenic tumor. → J Craniofac Surg. 2011 May;22(3):1151–7. 23. Jané-Salas E, López-López J, Roselló- Llabrés X, Rodríguez-Argueta OF, Chimenos-Küstner E. Relationship between oral cancer and implants: clinical cases and systematic literature review. → Med Oral Patol Oral Cir Bucal. 2012 Jan 1;17(1):e23–8.. The total number of patients was 34, and a total of 17 case reports were analyzed.
The patients were aged between 42 and 80 years (mean: 66.3 ± 10.1 years). Of all the case reports, 53% of the patients involved were men, while in the longitudinal randomized study, no significant differences regarding sex were found. An average of 4.58 ± 3.57 implants were placed per patient. In those documented case reports, a minimum of 2 implants were placed per patient, while in the longitudinal study, 56 implants were placed in 21 patients. The characteristics of those studies that meet the inclusion criteria are shown in Table 1.
Regarding the location, there was a clear predominance of the lower jaw (88.23%), specifically the posterior region (76.46%). The tumor was located on the lingual ridge in only 2 out of the 17 cases (11.77%). The average time between implant placement and diagnosis of OSCC was 0.25 months to 120 months (42.81 ± 37.73 months).
Prior to the implant placement, 76.47% of the patients presented 1 or more risk factors for developing a malignancy: 47.06% of cases had a previous history of oral carcinoma (squamous cells and verrucous carcinoma of the alveolar ridge) or cancer in other organs far from the oral cavity (lung cancer, pancreatic cancer or breast cancer); 11.76% had precancerous oral lesions, such as leukoplakia or lichen planus, while 35.3% had or used to have a tobacco addiction and 17.64% were regular alcohol consumers. In those cases considered for this review, OSCC developed very close to or directly in contact with the dental implants. In most of the cases, at the time of implant placement, there were 1 or more risk factors for the development of oral carcinoma.
Block and Scheufler in 2001 presented the case of a man aged 72, referred for the treatment of a progressive bone loss of 5 years of evolution surrounding 2 implants.42Block MS, Scheufler E. Squamous cell carcinoma appearing as peri-implant bone loss: a case report. → J Oral Maxillofac Surg. 2001 Nov;59(11):1349–52. This patient had proper oral hygiene and was a former smoker, having quit 16 years before, and had had a verrucous carcinoma removed from the alveolar bone of the lower jaw 3 years earlier. He had not undergone chemotherapy or radiotherapy. Two years later, after checking that the patient was in total remission, 2 implants had been placed in the left posterior region of his mandible. Six months later, the verrucous carcinoma reappeared on the periimplant mucosa. All of the affected tissue was removed, and a year later, 5 more implants were placed in order to support a fixed complete prosthesis. Five months after the placement of these implants, bone loss compatible with periimplantitis was found around 2 of the implants, with gingival hyperplasia and suppu ration. After performing a biopsy, a welldifferentiated OSCC was diagnosed. The 2 affected implants were removed, and after 18 months of follow-up, the patient was free of cancer and wore a removable prosthesis retained on the remaining implants.
Czerninski et al. in 2006 reported a case series in which implants were placed to replace missing teeth and ulcers appeared around these implants after several years after treatment.43Czerninski R, Kaplan I, Almoznino G, Maly A, Regev E. Oral squamous cell carcinoma around dental implants. → Quintessence Int. 2006 Oct;37(9):707–11. Histological analysis of these lesions confirmed the presence of OSCC surrounding the implants. The first case was of a 52-year-old woman, a smoker for more than 20 years, referred for treatment of oral lichen planus 8 years before. She had 3 implants, which had been placed 3 years before, and presented with a reddened mucosa surrounding the implants with ulcers of up to 25 mm on the alveolar ridge, initially diagnosed as periimplantitis. Radiographic examination showed bone loss surrounding the implants and a biopsy was done on which superficially invasive OSCC was diagnosed. Mandibulectomy and lymphatic node dissection were performed. After 18 months of follow-up, the patient was still free of cancer.
The second case was of an 80-year-old man with a history of diabetes and chronic ischemic heart disease. This patient had previously been treated for OSCC by resection, with no radiotherapy or combined treatment. On clinical examination, the patient had 5 dental implants, which had been placed 5 years earlier, in the anterior region of the mandible and presented with a partly ulcerated exophytic mass surrounding the implants of around 15 mm in diameter. The radiograph showed an osteolytic lesion with nondefined edges located lateral to the implants on the right of the patient’s mouth. Histological analysis confirmed OSCC affecting the mucosa and bone. This patient chose local extirpation of the tumor combined with palliative treatment and died a few months later because of cancer.44Czerninski R, Kaplan I, Almoznino G, Maly A, Regev E. Oral squamous cell carcinoma around dental implants. → Quintessence Int. 2006 Oct;37(9):707–11.
In 2008, Eguia del Valle et al. published the case of a man of 76 years of age who wore a fixed prosthesis supported on 2 implants located in the mandibular right region.45Eguia del Valle A, Martínez-Conde Llamosas R, López Vicente J, Uribarri Etxebarria A, Aguirre Urizar JM. Primary oral squamous cell carcinoma arising around dental osseointegrated implants mimicking peri-implantitis. → Med Oral Patol Oral Cir Bucal. 2008 Aug 1;13(8):E489–91. No toxic habits were present, and his general health was good. Three years after the implant placement, the patient presented with a white exophytic lesion of 6 mm in diameter and with superficial ulceration, located on the surrounding tissue of 1 of the implants. Radiographic examination showed cone-shaped bone loss surrounding this implant, and the biopsy confirmed the presence of a well-differentiated OSCC. Total resection of the tumor was performed, as well as lymphatic node dissection, but metastasis was not found.
Kwok et al. described in 2008 3 cases of OSCC in patients of 62, 71 and 67 years of age.46Kwok J, Eyeson J, Thompson I, McGurk M. Dental implants and squamous cell carcinoma in the at risk patient—report of three cases. → Br Dent J. 2008 Nov;205(10):543–5. All of them previously had risk factors for the development of oral cancer prior to the implant placement (previous oral carcinoma, previous breast cancer, smoking and alcohol use.
Gallego et al. published in 2009 a case of a 70-year-old woman who wore an overdenture supported on 3 dental implants.47Gallego L, Junquera L, Llorente S. Oral carcinoma associated with implant- supported overdenture trauma: a case report. → Dent Traumatol. 2009 Feb;25(1):e3–4. Her medical history provided no data of interest. The patient had an ulcerated lesion of 1 month of evolution located where the bar of the prosthesis pressed on the mucosa, close to 1 of the 3 implants. Biopsy confirmed a diagnosis of OSCC, requiring immediate removal of the bar and resection of part of the mandible. One year later, the patient was free of disease.
In 2009, Gulati et al. described the case of a female patient of 62 years of age and a heavy smoker (more than 20 cigarettes per day) who had been referred owing to a white lesion on the alveolar ridge at the mandibular left first molar.48Gulati A, Puthussery FJ, Downie IP, Flood TR. Squamous cell carcinoma presenting as peri-implantitis: a case report. → Ann R Coll Surg Engl. 2009 Oct;91(7):W8–10. Biopsy confirmed a diagnosis of well-differentiated OSCC, and a hemimandibulectomy was performed, plus radical dissection of neck nodes. One year later, implants were placed, but during the following 7 years, the patient suffered several episodes of periimplantitis of some of her implants. Several biopsies were done, all of them showed unspecific chronic inflammation, but no signs of dysplasia. However, 1 year later, another biopsy showed the presence of OSCC spread to the mouth floor. The treatment was radical dissection of the affected area, and 12 months later, 3 dental implants were placed in the anterior region. Again, 1 year after the implant placement, periimplantitis appeared again and biopsy confirmed the recurrence of the OSCC. Finally, the patient died because of other metastases.
The largest series of cases was published by De Ceulaer et al. in 2010.49De Ceulaer J, Magremanne M, van Veen A, Scheerlinck J. Squamous cell carcinoma recurrence around dental implants. → J Oral Maxillofac Surg. 2010 Oct;68(10):2507–12. Twenty-one patients were operated on with OSCC resection, and afterward implants were placed. In total, the patients had 56 implants placed. Sixteen of the patients had their implants placed in the same tumor resection surgery, and 5 of them in a second surgery. All of them underwent the same radiotherapy protocol. The results show that, in the group of implants placed in the same surgery, 3 patients had a tumor recurrence surrounding an implant; however, no recurrences were reported in the 2-stage surgery group.
Meijer et al. in 2010 reported the clinical case of a 69-year-old female patient with an overdenture on 2 mandibular anterior implants.50Meijer GJ, Dieleman FJ, Bergé SJ, Merkx MA. Removal of an oral squamous cell carcinoma including parts of osseointegrated implants in the marginal mandibulectomy. A case report. → Oral Maxillofac Surg. 2010 Dec;14(4):253–6. Eight years earlier, she had been operated on for resection of OSCC on the floor of the mouth, and in the same operation, several implants were placed to rehabilitate the area. Radiotherapy was necessary, and 3 months post-irradiation, prosthetic rehabilitation was performed. Four years after the prosthetic rehabilitation, a new tumor was detected around the adjacent keratinized tissue of both implants. Radiographically, there were no signs of osteolysis, and a partial mandibulectomy with the removal of both implants was performed. After 2 years, new implants were placed, and the patient was free of disease 1 year later.
Agostini et al. in 2011 reported a case that they referred to as periimplant squamous carcinoma.51Agostini T, Sacco R, Bertolai R, Acocella A, Colafranceschi M, Lazzeri D. Peri-implant squamous odontogenic tumor. → J Craniofac Surg. 2011 May;22(3):1151–7. 23. Jané-Salas E, López-López J, Roselló- Llabrés X, Rodríguez-Argueta OF, Chimenos-Küstner E. Relationship between oral cancer and implants: clinical cases and systematic literature review. → Med Oral Patol Oral Cir Bucal. 2012 Jan 1;17(1):e23–8. The person affected was a 64-year-old male patient with 3 implants in the mandibular left quadrant. Two months after placement, a painful radiolucency appeared close to the second premolar. A week later, there was a spontaneous failure of the implant and the pain had spread to the other 2. After the biopsy, OSCC was identified, and the corresponding resection carried out. After 7 years of follow-up, the patient showed no signs of recurrence.
Jané-Salas et al. in 2012 presented 2 cases. The first was of a 42-year-old male with a history of morbid obesity, but without toxic habits, who had had implants since 2007 in the mandibular posterior region.52Jané-Salas E, López-López J, Roselló- Llabrés X, Rodríguez-Argueta OF, Chimenos-Küstner E. Relationship between oral cancer and implants: clinical cases and systematic literature review. → Med Oral Patol Oral Cir Bucal. 2012 Jan 1;17(1):e23–8. The patient had no prosthesis on the implants and was examined owing to the presence of a painless ulcer or bleeding at the right edge of the tongue, which he attributed to self-injury and for which he refused a biopsy. In 2009, the ulcer persisted, and after the biopsy, OSCC was found. Hemimandibulectomy with lymphatic node resection was performed, and 6 months later, there was no evidence of recurrence of the lesion. The second case was of a 79-year-old man with no relevant history or toxic habits who had worn a complete maxillary denture on 7 implants for 9 years. The patient came to be examined because of the presence of an ulcer on the side of the tongue suspected to have arisen from trauma due to the fracture of ceramics of their maxillary rehabilitation. After 8 days, the ulcer had improved considerably, although soon after a biopsy of the ulcer, which was still present, the diagnosis of OSCC was confirmed. The patient underwent hemiglossectomy and functional dissection of lymphatic nodes. The patient remained free of disease after 2 years of follow-up.
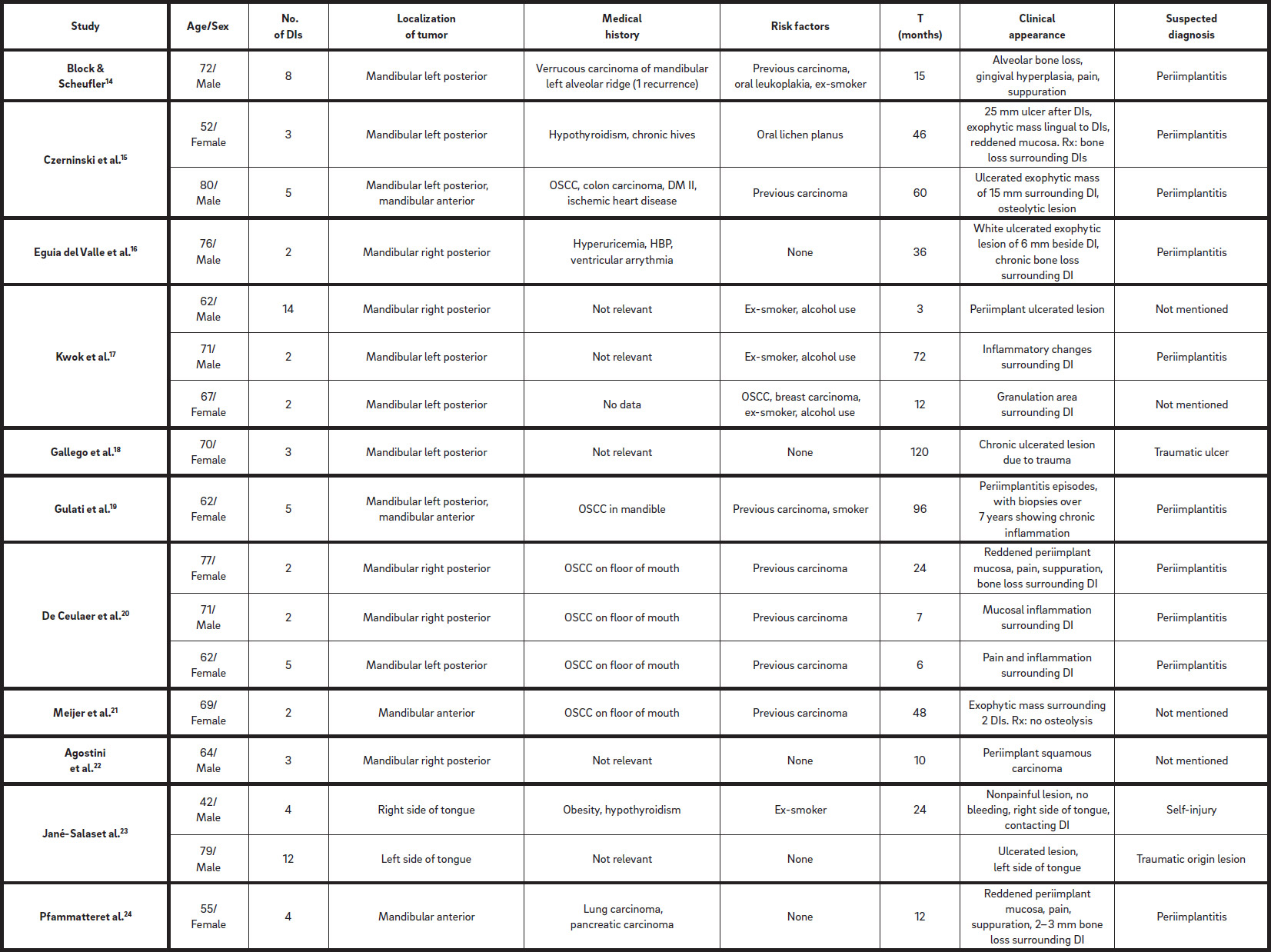
Table 1
Clinical cases from the articles included in this review.
Pfammatter et al. in 2012 presented the case of a 55-year-old woman with a history of pancreatic carcinoma who was referred by her dentist during chemotherapy owing to periimplantitis around an implant in the mandibular right anterior region.53Pfammatter C, Lindenmüller IH, Lugli A, Filippi A, Kühl S. Metastases and primary tumors around dental implants: a literature review and case report of peri-implant pulmonary metastasis. → Quintessence Int. 2012 Jul–Aug;43(7):563–70. The mucosa showed a smooth surface and typical signs of inflammation: pain, suppuration, erythema and a periodontal probing depth of 7 mm. Radiographic analysis showed distal and mesial bone loss of 2–3 mm around the implants in the mandibular anterior area. The area was mechanically debrided, and chlorhexidine and metronidazole gel were applied locally. Clinical signs decreased in the following 2 weeks, but 3 weeks later, the pain and suppuration appeared again and paresthesia of the lower lip was observed by the patient. Biopsy was performed in the implant area, revealing OSCC. The patient died 4 weeks after diagnosis.
Javed et al. in 2012 included in their review a total of 14 studies. Nine of these had a previous history of cancer, and 5 had toxic habits (tobacco and/or alcohol use).54Javed F, Al-Askar M, Qayyum F, Wang HL, Al-Hezaimi K. Oral squamous cell carcinoma arising around osseointegrated dental implants. → Implant Dent. 2012 Aug;21(4):280–6.
Discussion
Numerous studies have shown that dental implants can osseointegrate and remain functionally stable for long periods, both in healthy individuals and in medically compromised patients, including those who have undergone oncological therapy.55Buser D, Janner SF, Wittneben JG, Brägger U, Ramseier CA, Salvi GE. 10-year survival and success rates of 511 titanium implants with a sandblasted and acid-etched surface: a retrospective study in 303 partially edentulous patients. → Clin Implant Dent Relat Res. 2012 Dec;14(6):839–51.,56Jiang BQ, Lan J, Huang HY, Liang J, Ma XN, Huo LD, Xu X. A clinical study on the effectiveness of implant supported dental restoration in patients with chronic periodontal diseases. → Int J Oral Maxillofac Surg. 2013 Feb;42(2):256–9. doi:10.1016/j. ijom.2012.08.001. Epub 2012 Sep 26.,57Javed F, Al-Hezaimi K, Al-Rasheed A, Almas K, Romanos GE. Implant survival rate after oral cancer therapy: a review. → Oral Oncol. 2010 Dec;46(12):854–9.,58Bianchi B, Ferri A, Ferrari S, Leporati M, Copelli C, Ferri T, Sesenna E. Mandibular resection and reconstruction in the management of extensive ameloblastoma. → J Oral Maxillofac Surg. 2013 Mar;71(3):528–37. doi:10.1016/j. joms.2012.07.004. Epub 2012 Sep 27.,59Jacobsen C, Kruse A, Lübbers HT, Zwahlen R, Studer S, Zemann W, Seifert B, Grätz KW. Is mandibular reconstruction using vascularized fibula flaps and dental implants a reasonable treatment? → Clin Implant Dent Relat Res. 2014 Jun;16(3):419–28. doi:10.1111/ cid.12004. Epub 2012 Sep 21.,60Anne-Gaëlle B, Samuel S, Julie B, Renaud L, Pierre B. Dental implant placement after mandibular reconstruction by microvascular free fibula flap: current knowledge and remaining questions. → Oral Oncol. 2011 Dec;47(12):1099–104. However, although the evidence demonstrates the success of implant treatment in terms of survival,61Javed F, Al-Hezaimi K, Al-Rasheed A, Almas K, Romanos GE. Implant survival rate after oral cancer therapy: a review. → Oral Oncol. 2010 Dec;46(12):854–9.,62Jacobsen C, Kruse A, Lübbers HT, Zwahlen R, Studer S, Zemann W, Seifert B, Grätz KW. Is mandibular reconstruction using vascularized fibula flaps and dental implants a reasonable treatment? → Clin Implant Dent Relat Res. 2014 Jun;16(3):419–28. doi:10.1111/ cid.12004. Epub 2012 Sep 21.,63Carbiner R, Jerjes W, Shakib K, Giannoudis PV, Hopper C. Analysis of the compatibility of dental implant systems in fibula free flap reconstruction. → Head Neck Oncol. 2012 Jun 21;4:37. it is also true that there are numerous cases in the literature in which OSCC has been diagnosed around dental implants.64Block MS, Scheufler E. Squamous cell carcinoma appearing as peri-implant bone loss: a case report. → J Oral Maxillofac Surg. 2001 Nov;59(11):1349–52.,65Czerninski R, Kaplan I, Almoznino G, Maly A, Regev E. Oral squamous cell carcinoma around dental implants. → Quintessence Int. 2006 Oct;37(9):707–11.,66Eguia del Valle A, Martínez-Conde Llamosas R, López Vicente J, Uribarri Etxebarria A, Aguirre Urizar JM. Primary oral squamous cell carcinoma arising around dental osseointegrated implants mimicking peri-implantitis. → Med Oral Patol Oral Cir Bucal. 2008 Aug 1;13(8):E489–91.,67Kwok J, Eyeson J, Thompson I, McGurk M. Dental implants and squamous cell carcinoma in the at risk patient—report of three cases. → Br Dent J. 2008 Nov;205(10):543–5.,68Gallego L, Junquera L, Llorente S. Oral carcinoma associated with implant- supported overdenture trauma: a case report. → Dent Traumatol. 2009 Feb;25(1):e3–4.,69Gulati A, Puthussery FJ, Downie IP, Flood TR. Squamous cell carcinoma presenting as peri-implantitis: a case report. → Ann R Coll Surg Engl. 2009 Oct;91(7):W8–10.,70De Ceulaer J, Magremanne M, van Veen A, Scheerlinck J. Squamous cell carcinoma recurrence around dental implants. → J Oral Maxillofac Surg. 2010 Oct;68(10):2507–12.,71Meijer GJ, Dieleman FJ, Bergé SJ, Merkx MA. Removal of an oral squamous cell carcinoma including parts of osseointegrated implants in the marginal mandibulectomy. A case report. → Oral Maxillofac Surg. 2010 Dec;14(4):253–6.,72Agostini T, Sacco R, Bertolai R, Acocella A, Colafranceschi M, Lazzeri D. Peri-implant squamous odontogenic tumor. → J Craniofac Surg. 2011 May;22(3):1151–7. 23. Jané-Salas E, López-López J, Roselló- Llabrés X, Rodríguez-Argueta OF, Chimenos-Küstner E. Relationship between oral cancer and implants: clinical cases and systematic literature review. → Med Oral Patol Oral Cir Bucal. 2012 Jan 1;17(1):e23–8.,73Jané-Salas E, López-López J, Roselló- Llabrés X, Rodríguez-Argueta OF, Chimenos-Küstner E. Relationship between oral cancer and implants: clinical cases and systematic literature review. → Med Oral Patol Oral Cir Bucal. 2012 Jan 1;17(1):e23–8.,74Pfammatter C, Lindenmüller IH, Lugli A, Filippi A, Kühl S. Metastases and primary tumors around dental implants: a literature review and case report of peri-implant pulmonary metastasis. → Quintessence Int. 2012 Jul–Aug;43(7):563–70.,75Javed F, Al-Askar M, Qayyum F, Wang HL, Al-Hezaimi K. Oral squamous cell carcinoma arising around osseointegrated dental implants. → Implant Dent. 2012 Aug;21(4):280–6. Because of the multiple factors involved in the carcinogenesis process, it is very difficult to prove whether this relationship is purely coincidental or not.
Considering the cases evaluated in this review, several questions with difficult responses arise from current evidence: What exactly is the role of dental implants in the development of OSCC? And is it appropriate to treat a patient with implants if he or she has a previous history of carcinoma, premalignant lesions or another risk factor? Do implants alone increase the risk of the patient developing oral cancer?
OSCC around dental implants may present as a hyperplasic and/or ulcerated red zone of oral mucosa with alveolar bone loss, and is sometimes not distinguishable from periimplantitis when it develops around a prosthetic rehabilitation with dental implants, thereby presenting a possibility of misdiagnosis. Periimplantitis is a complication of implant treatment and typically shows alveolar bone loss around the affected implants, in addition to inflammation of the periimplant soft tissue.76Lindhe J, Meyle J; Group D of European Workshop on Periodontology. Peri-implant diseases: consensus report of the Sixth European Workshop on Periodontology. → J Clin Periodontol. 2008 Sep;35(8 Suppl):282–5. Since such inflammatory lesions around implants may manifest clinical and radiographic similarities to malignant diseases, in the case of gingival hyperplasia and/ or bone resorption around an implant, it is necessary to perform a thorough differential diagnosis. Under these circumstances, it is necessary to perform a detailed clinical and radiographic evaluation, accompanied by a biopsy and a histopathological test.
Thus, Block and Scheufler presented the case of a patient with periodontal bone loss around implants that initially was diagnosed as periimplantitis.77Block MS, Scheufler E. Squamous cell carcinoma appearing as peri-implant bone loss: a case report. → J Oral Maxillofac Surg. 2001 Nov;59(11):1349–52. The periimplant tissue that occupied the area of bone loss was debrided and sent for microscopic evaluation, and the histological results showed the presence of a well-differentiated OSCC.78Jané-Salas E, López-López J, Roselló- Llabrés X, Rodríguez-Argueta OF, Chimenos-Küstner E. Relationship between oral cancer and implants: clinical cases and systematic literature review. → Med Oral Patol Oral Cir Bucal. 2012 Jan 1;17(1):e23–8. The authors suggest that the likely sequence of OSCC development was from the soft tissue into the bone through the implants. The tumor had arisen in the soft tissue, and the implants had created a similar environment to the periodontal sulcus, facilitating the progression to bone.
A review of the literature from 1980–200579Czerninski R, Kaplan I, Almoznino G, Maly A, Regev E. Oral squamous cell carcinoma around dental implants. → Quintessence Int. 2006 Oct;37(9):707–11. found 4 articles describing 6 cases of OSCC associated with dental implants, which together with the 2 cases that the research group documented, brought the number to 8 cases. The mean age (72 years; range: 52–90 years) of the sample was higher than that of the present study (mean age: 66.3 ± 10.1 years), with a similar sex distribution. The location of the tumor was the lower jaw in all of the cases and only 1 of them had extension to the floor of the mouth. In the present review, there was also a clear predominance of mandibular occurrence (88.23%), particularly in the mandibular posterior area (76.46%) and mandibular anterior region (11.77%). Only in 2 out of the 17 cases did the tumor appear at the side of the tongue.
The etiology of OSCC is multifactorial, and it includes factors related to age, a previous history of oral and/or systemic cancer, toxic habits (tobacco and/or alcohol use) and infection with the human papillomavirus.80Hirota SK, Braga FP, Penha SS, Sugaya NN, Migliari DA. Risk factors for oral squamous cell carcinoma in young and older Brazilian patients: a comparative analysis. → Med Oral Patol Oral Cir Bucal. 2008 Apr;13(4):E227–31.,81Liang C, Marsit CJ, McClean MD, Nelson HH, Christensen BC, Haddad RI, Clark JR, Wein RO, Grillone GA, Houseman EA, Halec G, Waterboer T, Pawlita M, Krane JF, Kelsey KT. Biomarkers of HPV in head and neck squamous cell carcinoma. → Cancer Res. 2012 Oct;72(19):5004–13. Nutrition (diet high in fats and low in fruits and vegetables) and hygiene (poor oral hygiene) factors are also associated with an increased risk of oral cancer.82Hirota SK, Braga FP, Penha SS, Sugaya NN, Migliari DA. Risk factors for oral squamous cell carcinoma in young and older Brazilian patients: a comparative analysis. → Med Oral Patol Oral Cir Bucal. 2008 Apr;13(4):E227–31. Although OSCC may appear directly, it is usually preceded by premalignant oral lesions such as leukoplakia, erythroplakia or lichen planus.83Hirota SK, Braga FP, Penha SS, Sugaya NN, Migliari DA. Risk factors for oral squamous cell carcinoma in young and older Brazilian patients: a comparative analysis. → Med Oral Patol Oral Cir Bucal. 2008 Apr;13(4):E227–31. Czerninski et al. found that 87.5% of the evaluated patients had risk factors for developing oral carcinoma (a previous history of cancer [50.0%], premalignant lesions [25.0%] and toxic habits [25.0%]).15 The time between implant placement and tumor diagnosis varied from 0.5 years to 13 years (median: 4.5 years). Similar data were obtained in the present review, in which 76.47% of the patients had 1 or more risk factors for malignancy prior to placement of the dental implants, 47.06% of the cases had a history of oral carcinoma (OSCC and verrucous carcinoma of the alveolar ridge) or systemic cancer in other organs far from the oral cavity (lung cancer, pancreatic and breast), 11.76% had premalignant oral lesions (leukoplakia or lichen planus), 35.3% had or had had a smoking habit, and 17.64% were regular alcohol consumers. The average time between placement of the implants and diagnosis of OSCC in this review ranged between 0.25 months and 120 months (mean: 42 months). Smoking is the major known risk factor for the development of both premalignant oral lesions and oral cancer. It also has a negative effect on long-term implant success, as smoking cessation has shown significantly better outcomes.84Liddelow G, Klineberg I. Patient-related risk factors for implant therapy. A critique of pertinent literature. → Aust Dent J. 2011 Dec;56(4):417–26. There are reported cases in which the patient had no identified risk factor for developing oral carcinoma, and in all of them, the tumor was developed in close contact with the implants.85Gallego L, Junquera L, Llorente S. Oral carcinoma associated with implant- supported overdenture trauma: a case report. → Dent Traumatol. 2009 Feb;25(1):e3–4.,86Agostini T, Sacco R, Bertolai R, Acocella A, Colafranceschi M, Lazzeri D. Peri-implant squamous odontogenic tumor. → J Craniofac Surg. 2011 May;22(3):1151–7. 23. Jané-Salas E, López-López J, Roselló- Llabrés X, Rodríguez-Argueta OF, Chimenos-Küstner E. Relationship between oral cancer and implants: clinical cases and systematic literature review. → Med Oral Patol Oral Cir Bucal. 2012 Jan 1;17(1):e23–8.,87Jané-Salas E, López-López J, Roselló- Llabrés X, Rodríguez-Argueta OF, Chimenos-Küstner E. Relationship between oral cancer and implants: clinical cases and systematic literature review. → Med Oral Patol Oral Cir Bucal. 2012 Jan 1;17(1):e23–8. Some authors consider chronic trauma as resulting in a precancerous lesion if the cause of the trauma is not properly addressed.88Gallego L, Junquera L, Llorente S. Oral carcinoma associated with implant- supported overdenture trauma: a case report. → Dent Traumatol. 2009 Feb;25(1):e3–4.,89Pérez MA, Raimondi AR, Itoiz ME. An experimental model to demonstrate the carcinogenic action of oral chronic traumatic ulcer. → J Oral Pathol Med. 2005 Jan;34:17–22.
In all of the cases described but 1,90Meijer GJ, Dieleman FJ, Bergé SJ, Merkx MA. Removal of an oral squamous cell carcinoma including parts of osseointegrated implants in the marginal mandibulectomy. A case report. → Oral Maxillofac Surg. 2010 Dec;14(4):253–6. the tumor spread quickly into the bone and radiographic evidence of bone loss around the implant was found. OSCC begins in soft tissue and tends to invade the bone.91Johnson NW, Jayasekara P, Amarasinghe AA. Squamous cell carcinoma and precursor lesions of the oral cavity: epidemiology and aetiology. → Periodontol 2000. 2011 Oct;57(1):19–37.,92Rothenberg SM, Ellisen LW. The molecular pathogenesis of head and neck squamous cell carcinoma. → J Clin Invest. 2012 Jun;122(6):1951–7.
De Ceulaer et al. concluded that there is a higher recurrence of oral carcinoma in cases in which implants are placed in the same surgical procedure in which the tumor is removed.93De Ceulaer J, Magremanne M, van Veen A, Scheerlinck J. Squamous cell carcinoma recurrence around dental implants. → J Oral Maxillofac Surg. 2010 Oct;68(10):2507–12. They stated therefore that it would be advisable to wait for a second stage for implant placement once the tissue has healed and become stable.94De Ceulaer J, Magremanne M, van Veen A, Scheerlinck J. Squamous cell carcinoma recurrence around dental implants. → J Oral Maxillofac Surg. 2010 Oct;68(10):2507–12.
It is suggested that good periodontal health could provide a natural barrier against tumor progression, delaying bone infiltration.95Eguia del Valle A, Martínez-Conde Llamosas R, López Vicente J, Uribarri Etxebarria A, Aguirre Urizar JM. Primary oral squamous cell carcinoma arising around dental osseointegrated implants mimicking peri-implantitis. → Med Oral Patol Oral Cir Bucal. 2008 Aug 1;13(8):E489–91. Otherwise, the implant could provide an environment conducive to the rapid progression of the tumor to the bone in those cases in which the cancer originated in the epithelium of the adjacent mucosa.
In those cases in which the decision to place implants in a patient at high risk of developing oral carcinoma (smoking and a previous history of a tumor and/or premalignant lesion) is made, careful monitoring and appropriate clinical and radiographic follow-up will be indicated. The prosthesis should be designed to facilitate easy and regular removal, allowing regular control of the tissue.96Gallego L, Junquera L, Llorente S. Oral carcinoma associated with implant- supported overdenture trauma: a case report. → Dent Traumatol. 2009 Feb;25(1):e3–4.
Conclusion
In relation to the published evidence, definitive conclusions cannot be reached, although it can be said that, in patients with risk factors for oral carcinoma, an appropriate individualized risk– benefit assessment should be considered before making the decision to place implants.
In patients with risk factors who have been treated with dental implants, regular clinical and radiographic examination will be extremely necessary. The prosthesis should be designed to permit removal of plaque and facilitate adequate examination of the tissue. In the case of inflammatory changes or any kind of periimplant lesion, a biopsy should be taken and histopathologically analyzed urgently. In cases of patients who have developed an oral carcinoma, if implant placement is decided on, the surgery should be performed in a second phase, and not in the same tumor resection surgery, because a higher number of recurrences have been recorded for the latter.
Further studies are needed with larger series of cases and in collaboration with various cancer centers in order to explore further any direct relationship between OSCC and dental implants, as well as the possible role of the risk factors involved.
Competing interests
The authors declare that they have no competing interests.

Interview
with Ángela Rodríguez Caballero
Why did you conduct the research reported on in this paper?
For what reasons could others cite your paper?
How could your study’s findings have an impact on dentistry?
What is the relevance of your study’s findings to the daily practice of a dentist?
What are your recommendations for further investigation of the topic of your article?
References
| 1, 2. | ↑ | Ferlay J, Shin HR, Bray F, Formah D, Mathers C, Parkin DM. Estimates of worldwide burden of cancer in 2008: GLOBOCAN 2008. → Int J Cancer. 2010 Dec 15;127(12):2893–917. |
| 3, 4, 91. | ↑ | Johnson NW, Jayasekara P, Amarasinghe AA. Squamous cell carcinoma and precursor lesions of the oral cavity: epidemiology and aetiology. → Periodontol 2000. 2011 Oct;57(1):19–37. |
| 5, 92. | ↑ | Rothenberg SM, Ellisen LW. The molecular pathogenesis of head and neck squamous cell carcinoma. → J Clin Invest. 2012 Jun;122(6):1951–7. |
| 6, 7, 80, 82, 83. | ↑ | Hirota SK, Braga FP, Penha SS, Sugaya NN, Migliari DA. Risk factors for oral squamous cell carcinoma in young and older Brazilian patients: a comparative analysis. → Med Oral Patol Oral Cir Bucal. 2008 Apr;13(4):E227–31. |
| 8, 81. | ↑ | Liang C, Marsit CJ, McClean MD, Nelson HH, Christensen BC, Haddad RI, Clark JR, Wein RO, Grillone GA, Houseman EA, Halec G, Waterboer T, Pawlita M, Krane JF, Kelsey KT. Biomarkers of HPV in head and neck squamous cell carcinoma. → Cancer Res. 2012 Oct;72(19):5004–13. |
| 9, 55. | ↑ | Buser D, Janner SF, Wittneben JG, Brägger U, Ramseier CA, Salvi GE. 10-year survival and success rates of 511 titanium implants with a sandblasted and acid-etched surface: a retrospective study in 303 partially edentulous patients. → Clin Implant Dent Relat Res. 2012 Dec;14(6):839–51. |
| 10, 56. | ↑ | Jiang BQ, Lan J, Huang HY, Liang J, Ma XN, Huo LD, Xu X. A clinical study on the effectiveness of implant supported dental restoration in patients with chronic periodontal diseases. → Int J Oral Maxillofac Surg. 2013 Feb;42(2):256–9. doi:10.1016/j. ijom.2012.08.001. Epub 2012 Sep 26. |
| 11, 57, 61. | ↑ | Javed F, Al-Hezaimi K, Al-Rasheed A, Almas K, Romanos GE. Implant survival rate after oral cancer therapy: a review. → Oral Oncol. 2010 Dec;46(12):854–9. |
| 12, 58. | ↑ | Bianchi B, Ferri A, Ferrari S, Leporati M, Copelli C, Ferri T, Sesenna E. Mandibular resection and reconstruction in the management of extensive ameloblastoma. → J Oral Maxillofac Surg. 2013 Mar;71(3):528–37. doi:10.1016/j. joms.2012.07.004. Epub 2012 Sep 27. |
| 13, 59, 62. | ↑ | Jacobsen C, Kruse A, Lübbers HT, Zwahlen R, Studer S, Zemann W, Seifert B, Grätz KW. Is mandibular reconstruction using vascularized fibula flaps and dental implants a reasonable treatment? → Clin Implant Dent Relat Res. 2014 Jun;16(3):419–28. doi:10.1111/ cid.12004. Epub 2012 Sep 21. |
| 14, 60. | ↑ | Anne-Gaëlle B, Samuel S, Julie B, Renaud L, Pierre B. Dental implant placement after mandibular reconstruction by microvascular free fibula flap: current knowledge and remaining questions. → Oral Oncol. 2011 Dec;47(12):1099–104. |
| 15, 63. | ↑ | Carbiner R, Jerjes W, Shakib K, Giannoudis PV, Hopper C. Analysis of the compatibility of dental implant systems in fibula free flap reconstruction. → Head Neck Oncol. 2012 Jun 21;4:37. |
| 16, 17, 76. | ↑ | Lindhe J, Meyle J; Group D of European Workshop on Periodontology. Peri-implant diseases: consensus report of the Sixth European Workshop on Periodontology. → J Clin Periodontol. 2008 Sep;35(8 Suppl):282–5. |
| 18, 36, 42, 64, 77. | ↑ | Block MS, Scheufler E. Squamous cell carcinoma appearing as peri-implant bone loss: a case report. → J Oral Maxillofac Surg. 2001 Nov;59(11):1349–52. |
| 19, 30, 43, 44, 65, 79. | ↑ | Czerninski R, Kaplan I, Almoznino G, Maly A, Regev E. Oral squamous cell carcinoma around dental implants. → Quintessence Int. 2006 Oct;37(9):707–11. |
| 20, 37, 45, 66, 95. | ↑ | Eguia del Valle A, Martínez-Conde Llamosas R, López Vicente J, Uribarri Etxebarria A, Aguirre Urizar JM. Primary oral squamous cell carcinoma arising around dental osseointegrated implants mimicking peri-implantitis. → Med Oral Patol Oral Cir Bucal. 2008 Aug 1;13(8):E489–91. |
| 21, 35, 46, 67. | ↑ | Kwok J, Eyeson J, Thompson I, McGurk M. Dental implants and squamous cell carcinoma in the at risk patient—report of three cases. → Br Dent J. 2008 Nov;205(10):543–5. |
| 22, 38, 47, 68, 85, 88, 96. | ↑ | Gallego L, Junquera L, Llorente S. Oral carcinoma associated with implant- supported overdenture trauma: a case report. → Dent Traumatol. 2009 Feb;25(1):e3–4. |
| 23, 39, 48, 69. | ↑ | Gulati A, Puthussery FJ, Downie IP, Flood TR. Squamous cell carcinoma presenting as peri-implantitis: a case report. → Ann R Coll Surg Engl. 2009 Oct;91(7):W8–10. |
| 24, 34, 49, 70, 93, 94. | ↑ | De Ceulaer J, Magremanne M, van Veen A, Scheerlinck J. Squamous cell carcinoma recurrence around dental implants. → J Oral Maxillofac Surg. 2010 Oct;68(10):2507–12. |
| 25, 40, 50, 71, 90. | ↑ | Meijer GJ, Dieleman FJ, Bergé SJ, Merkx MA. Removal of an oral squamous cell carcinoma including parts of osseointegrated implants in the marginal mandibulectomy. A case report. → Oral Maxillofac Surg. 2010 Dec;14(4):253–6. |
| 26, 41, 51, 72, 86. | ↑ | Agostini T, Sacco R, Bertolai R, Acocella A, Colafranceschi M, Lazzeri D. Peri-implant squamous odontogenic tumor. → J Craniofac Surg. 2011 May;22(3):1151–7. 23. Jané-Salas E, López-López J, Roselló- Llabrés X, Rodríguez-Argueta OF, Chimenos-Küstner E. Relationship between oral cancer and implants: clinical cases and systematic literature review. → Med Oral Patol Oral Cir Bucal. 2012 Jan 1;17(1):e23–8. |
| 27, 31, 52, 73, 78, 87. | ↑ | Jané-Salas E, López-López J, Roselló- Llabrés X, Rodríguez-Argueta OF, Chimenos-Küstner E. Relationship between oral cancer and implants: clinical cases and systematic literature review. → Med Oral Patol Oral Cir Bucal. 2012 Jan 1;17(1):e23–8. |
| 28, 32, 53, 74. | ↑ | Pfammatter C, Lindenmüller IH, Lugli A, Filippi A, Kühl S. Metastases and primary tumors around dental implants: a literature review and case report of peri-implant pulmonary metastasis. → Quintessence Int. 2012 Jul–Aug;43(7):563–70. |
| 29, 33, 54, 75. | ↑ | Javed F, Al-Askar M, Qayyum F, Wang HL, Al-Hezaimi K. Oral squamous cell carcinoma arising around osseointegrated dental implants. → Implant Dent. 2012 Aug;21(4):280–6. |
| 84. | ↑ | Liddelow G, Klineberg I. Patient-related risk factors for implant therapy. A critique of pertinent literature. → Aust Dent J. 2011 Dec;56(4):417–26. |
| 89. | ↑ | Pérez MA, Raimondi AR, Itoiz ME. An experimental model to demonstrate the carcinogenic action of oral chronic traumatic ulcer. → J Oral Pathol Med. 2005 Jan;34:17–22. |





Leave a Reply
Be the First to Comment!