Trends in clinical trials on bone regeneration in dentistry—towards an innovative development in dental implant treatment
January 7, 2020 / Categories: Digital Dentistry, Implant Dentistry

Yamada, Yoichi
Nakamura-Yamada, Sayaka
Miki, Michihide
Nakajima, Yasushi

Baba, Shunsuke
Abstract
Objective
The aim of this study was to assess the global trends in clinical trials on bone regeneration in dental implantology.
Materials and methods
An electronic search for clinical studies was conducted via the ClinicalTrials.gov database. The search strategy used the following terms: “bone regeneration” AND “oral,” and “bone regeneration” AND “dental”. Furthermore, the selected clinical studies were resurveyed using “bone regeneration” AND “dental implant,” and “bone regeneration” AND “oral” AND “implant” for further analysis.
Results
We selected 181 clinical studies related to the field of bone regeneration in dentistry from ClinicalTrials.gov. The selected studies were conducted in 27 countries from 2001 to the present, and the total number of studies has been increasing since 2011. Analysis of the clinical stage revealed a higher ratio (55.6%) of early study phases (early phase 1, phase 1, phase 1/2 and phase 2), but the periodontal field of application appeared more mature, having more phase 4 trials. Regarding the bone regeneration methods for dental implantology, the major technique examined in interventional clinical trials was guided bone regeneration, followed by alveolar ridge preservation, and sinus floor elevation. Various grafting materials, such as autografts, allografts, xenografts, alloplasts and barrier membranes, were examined to determine clinical efficacy. Combinations of these materials were more frequently used.
Conclusion
Our analysis of the clinical trials registered on the ClinicalTrials. gov database indicated the global clinical trends in bone regeneration techniques in dentistry. The randomized clinical trials of guided bone regeneration technique using combination of different bone grafts materials is conducted the most in dental implantology. These findings could be useful for development of an innovative therapy for bone regeneration.
Keywords
Bone regeneration; clinical trials; Clinical- Trials.gov; dental implants; regenerative medicine.
Introduction
A clinical trial is a study in humans that assesses safety and effectiveness of a new treatment. It is essential to develop new treatment for therapeutic use. It is clearly crucial to conduct clinical trials and log the relevant information on a database for development of novel medicine. During the 1990s, clinical trial registration was strongly promoted in biomedical research, with the aim of documenting the existence of all trials and eliminating publication bias. The International Committee of Medical Journal Editors required registration of all trials starting enrollment after July 1, 2005, and of ongoing clinical trials that began enrolling patients before that date.1Dickersin K, Rennie D. The evolution of trial registries and their use to assess the clinical trial enterprise. → JAMA. 2012 May 2;307(17):1861–4. The World Health Organization declared support for clinical trial registration and in 2006 launched the WHO International Clinical Trials Registry Platform (ICTRP)2International Clinical Trials Registry Platform Search Portal [Internet]. Version 3.6. → Geneva: World Health Organization. c2006 – [cited 2019 Nov 24]. Available from: http://apps.who.int/trialsearch/.. The Clinical Trials Search Portal provides access to a central database containing the trial registration datasets. Currently, there are 17 data providers of the ICTRP Search Portal, including ClinicalTrials.gov, the EU Clinical Trials Register, the ISRCTN registry, the Japan Primary Registries Network, the Australian New Zealand Clinical Trials Registry, the Brazilian Clinical Trials Registry and the Chinese Clinical Trial Register (https://www.who.int/ ictrp/search/data_providers/en/).
ClinicalTrials.gov is a database of privately and publicly funded clinical studies conducted around the world and is the world’s largest clinical trial registration database. It is hosted by the National Library of Medicine at the National Institutes of Health in collaboration with the U.S. Food and Drug Administration. It explores 321,732 research studies in 209 countries and provides information about target diseases, sponsors, principal investigators, planned schedules and protocols, and enrollment. Moreover, since the database provides comprehensive information on the content of the planned clinical trials, one can perform various targeted analyses by extracting and tagging attribute data from each clinical study plan.3Negoro T, Takagaki Y, Okura H, Matsuyama A. Trends in clinical trials for articular cartilage repair by cell therapy. → NPJ Regen Med. 2018 Oct 11;3:17. doi: 10.1038/s41536-018-0055-2.
Alveolar bone loss is often caused by trauma, pathology, chronic or acute infections, severe periodontitis, and loss of mechanical function after tooth extraction or tooth loss.4Sanz-Sánchez I, Ortiz-Vigón A, Sanz-Martín I, Figuero E, Sanz M. Effectiveness of lateral bone augmentation on the alveolar crest dimension: A systematic review and meta-analysis. → J Dent Res. 2015 Sep;94(9 Suppl):128S–42S. Since the overall alveolar changes after tooth extraction may compromise prosthodontic rehabilitation using tooth-supported fixed or removable prostheses, as well as implant-supported prostheses, adequate quality and quantity of bone regeneration are required, especially in the field of implant dentistry.5Atieh MA, Alsabeeha NH, Payne AG, Duncan W, Faggion CM, Esposito M. Interventions for replacing missing teeth: alveolar ridge preservation techniques for dental implant site development. → Cochrane Database Syst Rev. 2015 May 28;(5):CD010176. doi: 10.1002/14651858. CD010176.pub2. Various materials and surgical treatments have been developed, but a definitive bone regeneration technique is not yet established. To the best of our knowledge, there are no scientific reports that have comprehensively analyzed and examined the clinical research trends in bone regeneration in dental implant treatment.
In this article, the focus was on bone regeneration for an innovative development in dental implant treatment based on the clinical trials registration database. Since ClinicalTrials.gov is the largest clinical trial registration database in the world and is one of the best designed database providers for aggregation and analysis,6Tasneem A, Aberle L, Ananth H, Chakraborty S, Chiswell K, McCourt BJ, Pietrobon R. The database for aggregate analysis of ClinicalTrials.gov (AACT) and subsequent regrouping by clinical specialty. → PLOS ONE. 2012;7(3):e33677. doi: 10.1371/journal.pone.0033677. we chose it to obtain the data for analysis. In this concise review, we first surveyed country, start year and clinical stage of clinical studies on bone regeneration in dentistry to identify global translational trends and followed this with analysis of the details about clinical trials in dental implantology. We aimed to establish global translational trends, which have thus far been difficult to interpret. The results of this study could be useful to learn of the development of new techniques in dental implantology.
Materials and methods
In this review, an extensive electronic search for clinical studies was conducted via the ClinicalTrials.gov database. The last search was updated on Nov. 11, 2019. Medical Subject Headings, combined with free words, was used to identify the search terms. The following search terms: “bone regeneration” AND “oral,” and “bone regeneration” AND “dental” were used for analysis by country, start year and clinical stage of the clinical studies. In this survey, we excluded duplicate studies and in vitro or preclinical studies using human subjects. In clinical stage analysis, the studies that were described as “not applicable” in the database were excluded. Furthermore, the selected clinical studies were resurveyed using “bone regeneration” AND “dental implant,” and “bone regeneration” AND “oral” AND “implant.” We excluded studies that were not related to bone regeneration by reading the descriptions of the individual studies.
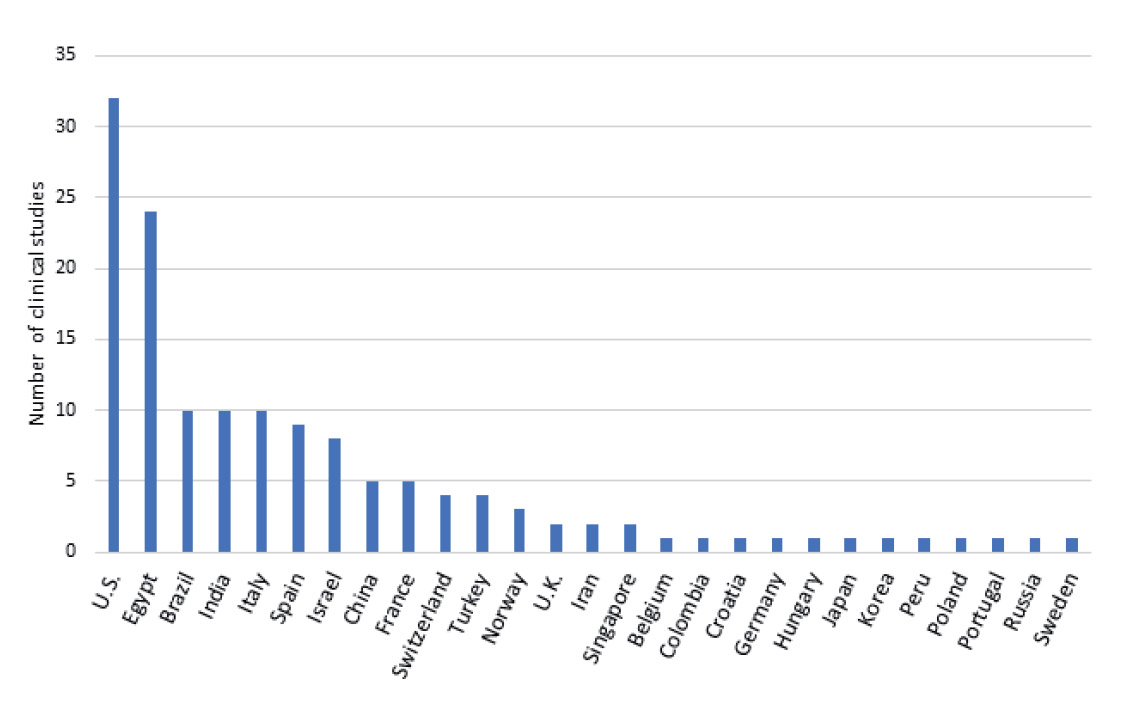
Fig. 1
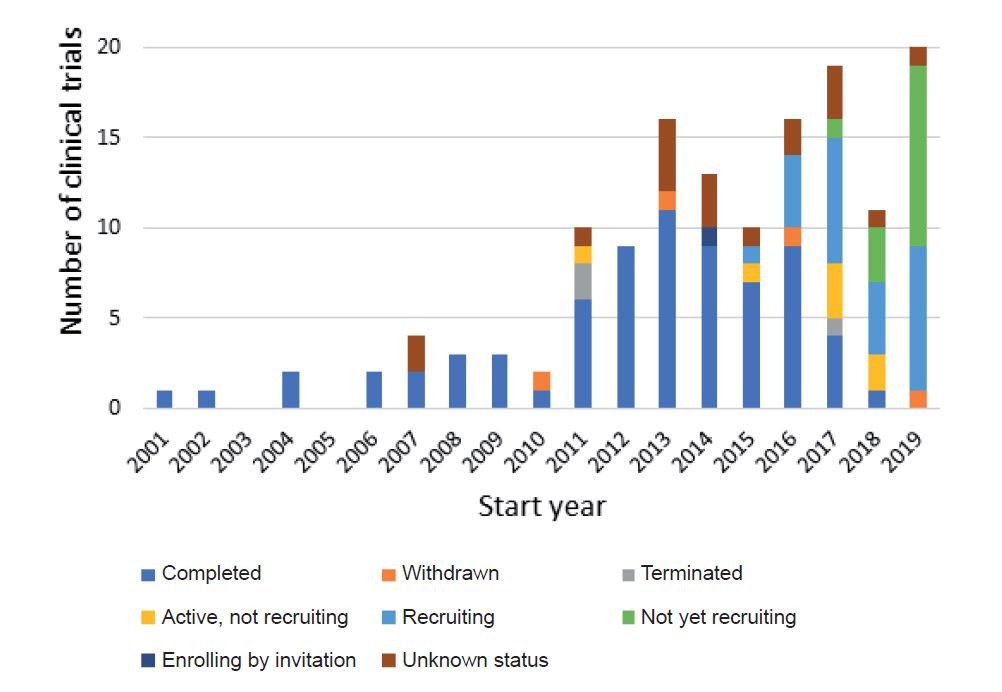
Fig. 2
Results
We first surveyed ClinicalTrials.gov to identify translational trends in bone regeneration in dentistry. Initially, 181 studies were selected through a primary database search. After excluding duplicate studies, 144 studies remained. We excluded in vitro or preclinical studies using human subjects by carefully reading the descriptions of the individual studies, and 142 studies were used for their content for analysis. First, we classified the entire list of clinical studies on bone regeneration in dentistry by country (Fig. 1). The selected clinical studies were conducted in 27 countries, and the major country was the U.S. (32 studies), followed by Egypt (24 studies), Brazil (10 studies), India (10 studies), and Italy (10 studies).
In order to analyze the clinical research trends regarding bone regeneration in dentistry, the selected studies were sorted by start year (Fig. 2). This analysis showed that bone regeneration therapy was performed in dentistry from 2001 to the present. The first study was a clinical trial on periodontal tissue regeneration using fibroblast growth factor-2 conducted in Japan. The total number of studies has been increasing since 2011. The clinical studies were classified according to their current status. Some studies were withdrawn and the reasons given were the following “Principal investigator and sponsor did not reach an agreement,” “Lack of pediatric recruitment ability,” “Administrative changes precluded enrollment,” and “It was not approved by IRB [institutional review board].”
To determine progress in testing novel methods of bone regeneration in dentistry, the clinical stage was analyzed (Fig. 3). Among the selected studies, 79 studies were not applicable. Early phase 1, phase 1, phase 1/2 and phase 2 studies made up 55.6% of bone regeneration studies in dentistry. There were 17 phase 4 clinical trials, 9 of which were conducted in order to evaluate the efficacy of various products in the treatment of periodontal bone defects.
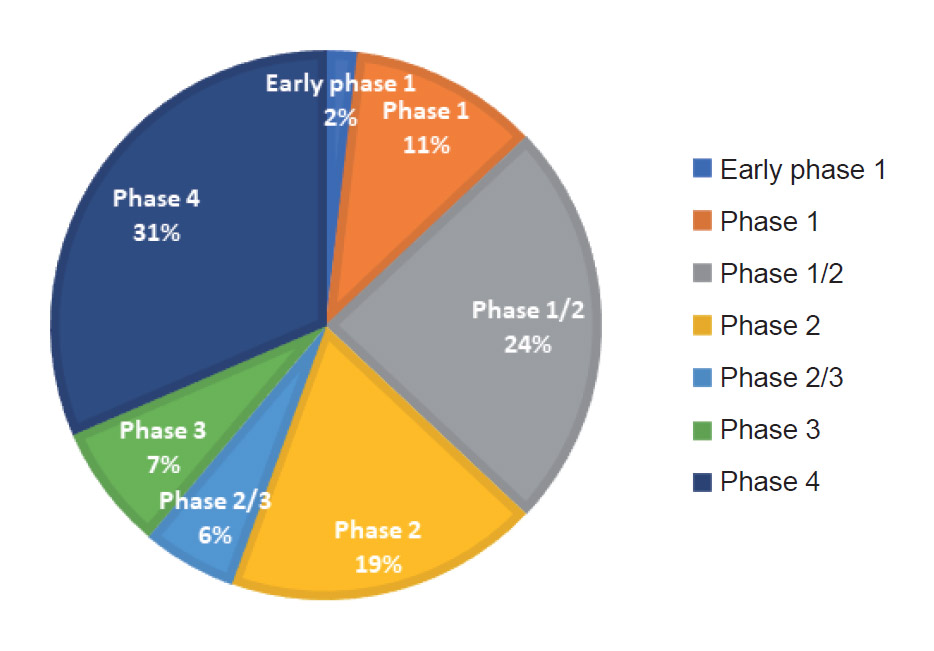
Fig. 3
-
- Fig. 4a
-
- Fig. 4b
The products used in periodontal treatment were as follows: atorvastatin gel, biological amniotic membrane, rosuvastatin, decalcified freeze-dried bone allograft and cerabone bone (botiss biomaterials), alendronate, simvastatin gel, amnion–chorion allograft membrane, and biphasic calcium phosphate (Straumann BoneCeramic, Straumann) combined with enamel matrix proteins (Straumann Emdogain, Straumann). Guided bone regeneration (GBR) using autografts (autogenous dentinal graft), allografts (enCore Combination Allograft [Osteogenics Biomedical], cancellous block allograft plus a demineralized bone matrix allograft [Optecure +ccc, Exactech]), and xenografts (deproteinized bovine bone mineral [Geistlich Bio-Oss, Geistlich]) and collagen membranes (Geistlich Bio-Gide) was also evaluated in phase 4 clinical trials.
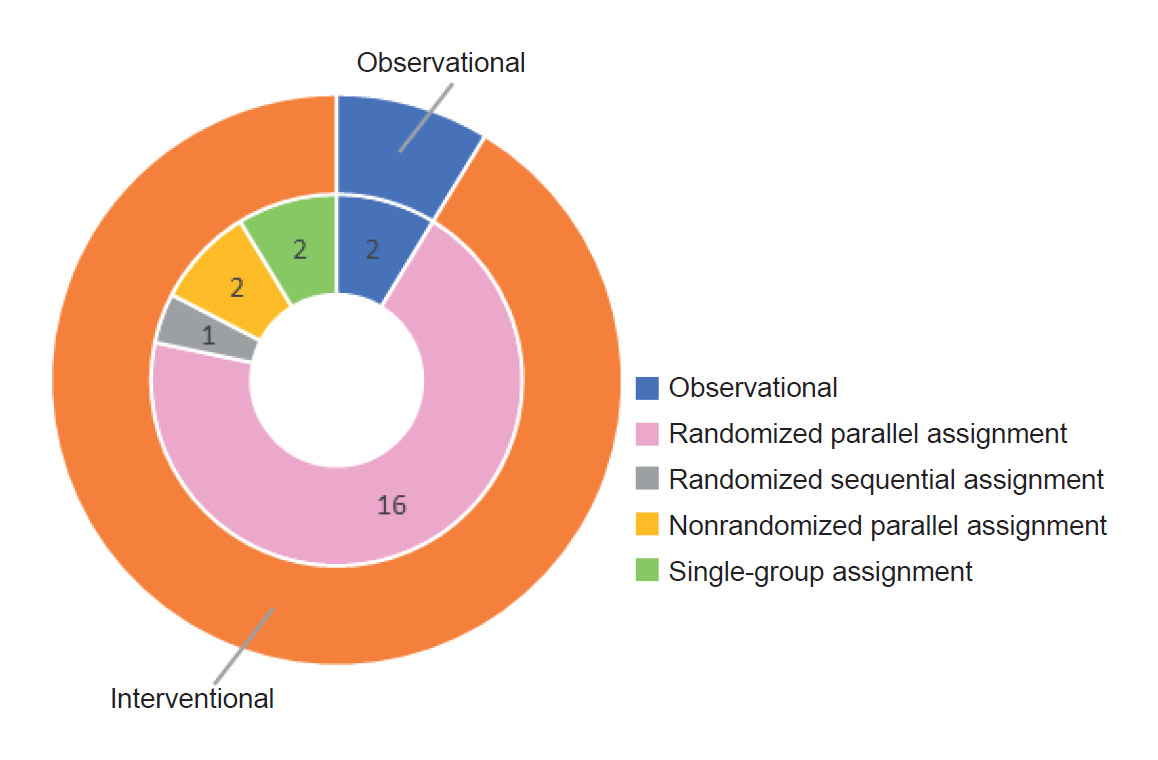
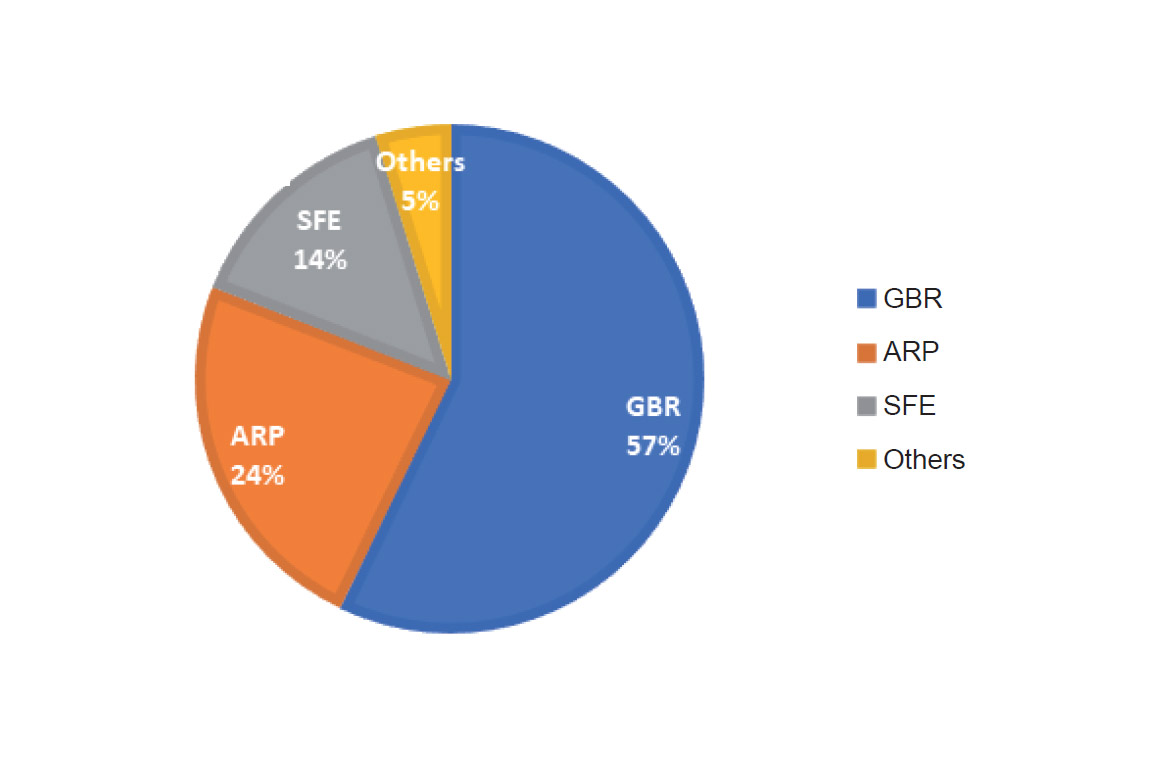
In the next step, we focused on bone regeneration studies in patients requiring dental implant placement. Twenty-four studies were selected through a database search, and 1 study was excluded because the technique was aimed at periimplantitis treatment not bone regeneration. In total, 23 studies were used for the analyses. The number of clinical studies according to study design is shown in Figure 4A. Most of them were interventional studies (21 studies). An overview of the interventional clinical trials on bone regeneration in dental implantology is shown in Table 1. Among these interventional studies, 16 were parallel design randomized controlled trials. Regarding the bone regeneration methods, the major technique examined in interventional clinical trials was GBR (12 studies), followed by alveolar ridge preservation (ARP; 5 studies), and sinus floor elevation (SFE; 3 studies; Fig. 4B). The characteristics of the interventions are shown in Table 2. The results indicated that various grafting materials and procedures were examined to determine clinical efficacy. The grafting materials included autografts (bone marrow-derived cells, dentinal graft and platelet-rich fibrin), allografts (freeze-dried bone allograft, cortico-cancellous allogeneic block [PHOENIX, TBF] and MinerOss [BioHorizons], xenografts (deproteinized bovine bone mineral [Geistlich Bio-Oss]), and alloplasts (biphasic calcium sulfate [BONDBONE, MIS Implant Technologies], calcium phosphosilicate alloplastic bone and nanocrystalline synthetic hydroxyapatite [NanoBone, ARTOSS]). Combinations of these materials were more frequently used (5 studies). The usefulness of membranes was also examined for the GBR and ARP techniques.
Discussion
In general, a new treatment should go through several procedures before it will be approved for therapeutic use. After tests and treatments are assessed in preclinical research, they go through a series of clinical trials in humans. To date, there are no clear reports on comprehensive clinical development trends in specific fields of regenerative medicine using a clinical trial registry. In this study, we focused on bone regeneration in dentistry, especially in dental implantology, based on the data obtained from ClinicalTrials.gov. We used data available on the ClinicalTrials.gov registry as the primary source in order to conduct comprehensive and chronological research, classification and analysis of clinical trials registered in this field, including assessing global research trends in bone regeneration. The clinical trials were conducted all over the world. Although ClinicalTrials.gov is the most global database in the world, there are other data providers. Since clinical trials tend to be registered in the database of their own country, many studies in the U.S. might be registered on ClinicalTrials.gov, but fewer studies in Japan, Australia or Germany, among others, might be registered.
Generally, clinical trials have 4 phases: phases 1–4. Phase 0/early phase 1 has been introduced to assist in eliminating ineffective products early in the development process and is not considered to replace formal phase 1 safety and tolerance studies.7Therapeutic Goods Administration (AU). Australian clinical trial handbook: guidance on conducting clinical trials in Australia using ‘unapproved’ therapeutic goods. Version 2.2. → Woden: Therapeutic Goods Administration; 2018. 61 p. Phase 1 trials may involve the first administration to humans, usually to small numbers of healthy volunteers or to patients, in order to test safety and tolerance. If a new treatment is found to be reasonably safe in a phase 1 clinical trial, it can then be tested in a phase 2 clinical trial to find out whether it works. Phase 2 trials may be undertaken in a larger group of human patients to further assess safety and efficacy. Treatments that have been shown to work in phase 2 studies usually must succeed in 1 more phase of testing (phase 3) before they are approved for general use. Phase 3 trials usually involve a large group of patients, in order to compare the safety and effectiveness of the new treatment against the current standard treatment. When a phase 3 clinical trial (or sometimes a phase 2 trial) shows that a new treatment is more effective and/ or safer than the current standard one, it can be submitted for approval. Our results indicated a higher ratio of early study phases (early phase 1, phase 1, phase 1/2 and phase 2) in the field of bone regeneration. The periodontal field of application appeared more mature, having more phase 4 studies. In the U.S., more than 47% people ≥ 30 years of age have periodontal disease, and the prevalence increases to 70% among those of ≥ 65 years of age.8Lamster IB, Pagan M. Periodontal disease and the metabolic syndrome. → Int Dent J. 2017 Apr;67(2):67–77. A similar trend is found in other countries. 9Lamster IB, Pagan M. Periodontal disease and the metabolic syndrome. → Int Dent J. 2017 Apr;67(2):67–77.,10Albandar JM. Global epidemiology and risk factors of periodontal diseases, and preliminary assessment of the periodontal status in Japan. → J Jpn Health Care Dental Association. 2004;6:42–55. Since there is a strong need for periodontal treatment, clinical trials in periodontitis might be accelerated.

Table 1: Overview of clinical trials on bone regeneration in dental implantology.
‡ DBBM = deproteinized bovine bone mineral.
§ GBR = guided bone regeneration.
†† PEG = polyethylene glycol.
‡‡ PRF = platelet-rich fibrin.
§§ VEGF = vascular endothelial growth factor.
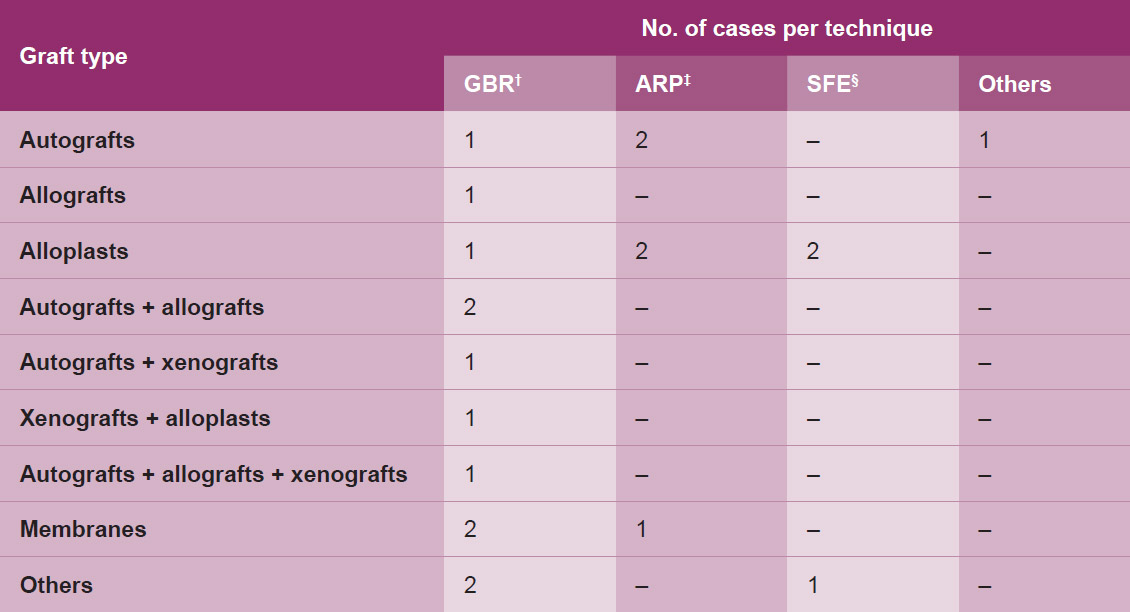
Table 2: Characteristics of interventions.
† GBR = guided bone regeneration.
‡ ARP = alveolar ridge preservation.
§ SFE = sinus floor elevation.
A randomized controlled clinical trial is a study design that uses control patients who receive no treatment, the conventional treatment or a placebo. Randomization is the best way of ensuring that the results of trials are not biased by the way participants in each group are selected, so randomized controlled trials are the most reliable way to compare treatments. In this study, of the 23 trials on bone regeneration in dental implantology screened, 21 studies were interventional studies, 17 of which employed randomized assignment. The results indicated that the rate of randomized assignment was high (73.9%) in dental implantology studies.
Loss of bone width and depth can affect how successful the implant will be. In order to regenerate adequate bone volume for dental implant placement, the GBR technique is often performed. Most studies aiming for lateral bone augmentation have used the principles of GBR by combining different bone grafts and barrier membranes.11Sanz-Sánchez I, Ortiz-Vigón A, Sanz-Martín I, Figuero E, Sanz M. Effectiveness of lateral bone augmentation on the alveolar crest dimension: A systematic review and meta-analysis. → J Dent Res. 2015 Sep;94(9 Suppl):128S–42S. However, the ideal graft or membrane material remains unclear.12Sanz-Sánchez I, Ortiz-Vigón A, Sanz-Martín I, Figuero E, Sanz M. Effectiveness of lateral bone augmentation on the alveolar crest dimension: A systematic review and meta-analysis. → J Dent Res. 2015 Sep;94(9 Suppl):128S–42S. The results of our study indicated that 57% of interventional clinical trials on bone regeneration in dental implantology (12 studies) used the GBR technique. Most studies on GBR treatment (41.7%) combined different bone grafts: autografts and allografts; autografts and xenografts; xenografts and alloplasts; and autografts, allografts and xenografts.
In humans, approximately 50% of the bone volume is lost after tooth extraction during the first year.13Schropp L, Kostopoulos L, Wenzel A. Bone healing following immediate versus delayed placement of titanium implants into extraction sockets: a prospective clinical study. → Int J Oral Maxillofac Implants. 2003 Mar–Apr;18(2):189–99.,14Tan WL, Wong TL, Wong MC, Lang NP. A systematic review of post-extractional alveolar hard and soft tissue dimensional changes in humans. → Clin Oral Implants Res. 2012 Feb;23 Suppl 5:1–21. The alveolar bone resorption may not allow optimal positioning of dental implants.15John V, De Poi R, Blanchard S. Socket preservation as a precursor of future implant placement: review of the literature and case reports. → Compend Contin Educ Dent. 2007 Dec;28(12):646–53; quiz 654, 671.,16Mecall RA, Rosenfeld AL. Influence of residual ridge resorption patterns on implant fixture placement and tooth position. → Int J Periodontics Restorative Dent. 1991;11(1):8–23. Maxillary sinus floor augmentation via SFE is a surgical procedure to gain the bone mass required in order to place dental implants. There is consensus that some threshold of osseous deficiency, vertical, horizontal or both, exists at a site where a sinus bone graft is required for successful implant treatment regardless of residual bone quality.17Yamada Y, Nakamura S, Ito K, Kohgo T, Hibi H, Nagasaka T, Ueda M. Injectable tissue-engineered bone using autogenous bone marrow-derived stromal cells for maxillary sinus augmentation: clinical application report from a 2–6-year follow-up. → Tissue Eng Part A. 2008 Oct;14(10):1699–707. Although this procedure is considered safe, various complications may arise during or after the surgery, such as perforation of the sinus membrane.18Tükel HC, Tatli U. Risk factors and clinical outcomes of sinus membrane perforation during lateral window sinus lifting: analysis of 120 patients. → Int J Oral Maxillofac Surg. 2018 Sep;47(9):1189–94. ARP is performed after tooth extraction in an attempt to maintain the alveolar ridge height and width. ARP is a less invasive technique than SFE. The results of this study showed that the start dates of SFE clinical trials were from 2004 to 2013, whereas those of ARP studies were from 2006 to 2017. These results indicated a shift from SFE to ARP for bone regeneration in dental implantology.
In this study, we utilized the most global clinical trial database, ClinicalTrials.gov, to capture the largest trends in bone regeneration studies in dental implantology. The limitation of this study is that registered trials make up only a part of all existing trials. It has been suggested that only 50% of clinical studies indexed in PubMed that involved administration of cells for regenerative medicine indicated any clinical trial identifier.19Monsarrat P, Vergnes JN, Planat-Bénard V, Ravaud P, Kémoun P, Sensebé L, Casteilla L. An innovative, comprehensive mapping and multiscale analysis of registered trials for stem cell-based regenerative medicine. → Stem Cells Transl Med. 2016 Jun;5(6):826–35. In addition, since ClinicalTrials.gov does not provide comprehensive results of clinical trials, it is impossible to analyze the results of the trials themselves.
Conclusion
In conclusion, these results on clinical trials registered on the ClinicalTrials.gov registration site showed the global trends in clinical trials on bone regeneration in implant dentistry. ClinicalTrials.gov, a publicly accessible database, is useful for detailed characterization and analysis of clinical trials. This study revealed that the periodontal field of application was more accelerated, having more phase 4 studies. As for implant dentistry, the most frequently conducted study was the randomized clinical trials of GBR technique using combination of different bone grafts materials. The present study has potential implications for understanding the clinical trends in the development of therapeutic bone regeneration techniques in dental implantology. In the future, further studies would be needed for further development of an innovative therapy in dental implant treatment.
Competing interests
The authors declare that they have no competing interests.
Figure legends
Fig. 1 – The number of clinical trials on bone regeneration in dentistry according to country.
Fig. 2 – The number of clinical trials on bone regeneration in dentistry according to start year. The current status of the studies is also color-coded.
Fig. 3 – Phases of clinical trials on bone regeneration in dentistry.
Fig. 4 – Study design (A) and bone regeneration method (B) of clinical trials on bone regeneration in dental implantology. GBR = guided bone regeneration; ARP = alveolar ridge preservation; SFE = sinus floor elevation.
References
| 1. | ↑ | Dickersin K, Rennie D. The evolution of trial registries and their use to assess the clinical trial enterprise. → JAMA. 2012 May 2;307(17):1861–4. |
| 2. | ↑ | International Clinical Trials Registry Platform Search Portal [Internet]. Version 3.6. → Geneva: World Health Organization. c2006 – [cited 2019 Nov 24]. Available from: http://apps.who.int/trialsearch/. |
| 3. | ↑ | Negoro T, Takagaki Y, Okura H, Matsuyama A. Trends in clinical trials for articular cartilage repair by cell therapy. → NPJ Regen Med. 2018 Oct 11;3:17. doi: 10.1038/s41536-018-0055-2. |
| 4, 11, 12. | ↑ | Sanz-Sánchez I, Ortiz-Vigón A, Sanz-Martín I, Figuero E, Sanz M. Effectiveness of lateral bone augmentation on the alveolar crest dimension: A systematic review and meta-analysis. → J Dent Res. 2015 Sep;94(9 Suppl):128S–42S. |
| 5. | ↑ | Atieh MA, Alsabeeha NH, Payne AG, Duncan W, Faggion CM, Esposito M. Interventions for replacing missing teeth: alveolar ridge preservation techniques for dental implant site development. → Cochrane Database Syst Rev. 2015 May 28;(5):CD010176. doi: 10.1002/14651858. CD010176.pub2. |
| 6. | ↑ | Tasneem A, Aberle L, Ananth H, Chakraborty S, Chiswell K, McCourt BJ, Pietrobon R. The database for aggregate analysis of ClinicalTrials.gov (AACT) and subsequent regrouping by clinical specialty. → PLOS ONE. 2012;7(3):e33677. doi: 10.1371/journal.pone.0033677. |
| 7. | ↑ | Therapeutic Goods Administration (AU). Australian clinical trial handbook: guidance on conducting clinical trials in Australia using ‘unapproved’ therapeutic goods. Version 2.2. → Woden: Therapeutic Goods Administration; 2018. 61 p. |
| 8, 9. | ↑ | Lamster IB, Pagan M. Periodontal disease and the metabolic syndrome. → Int Dent J. 2017 Apr;67(2):67–77. |
| 10. | ↑ | Albandar JM. Global epidemiology and risk factors of periodontal diseases, and preliminary assessment of the periodontal status in Japan. → J Jpn Health Care Dental Association. 2004;6:42–55. |
| 13. | ↑ | Schropp L, Kostopoulos L, Wenzel A. Bone healing following immediate versus delayed placement of titanium implants into extraction sockets: a prospective clinical study. → Int J Oral Maxillofac Implants. 2003 Mar–Apr;18(2):189–99. |
| 14. | ↑ | Tan WL, Wong TL, Wong MC, Lang NP. A systematic review of post-extractional alveolar hard and soft tissue dimensional changes in humans. → Clin Oral Implants Res. 2012 Feb;23 Suppl 5:1–21. |
| 15. | ↑ | John V, De Poi R, Blanchard S. Socket preservation as a precursor of future implant placement: review of the literature and case reports. → Compend Contin Educ Dent. 2007 Dec;28(12):646–53; quiz 654, 671. |
| 16. | ↑ | Mecall RA, Rosenfeld AL. Influence of residual ridge resorption patterns on implant fixture placement and tooth position. → Int J Periodontics Restorative Dent. 1991;11(1):8–23. |
| 17. | ↑ | Yamada Y, Nakamura S, Ito K, Kohgo T, Hibi H, Nagasaka T, Ueda M. Injectable tissue-engineered bone using autogenous bone marrow-derived stromal cells for maxillary sinus augmentation: clinical application report from a 2–6-year follow-up. → Tissue Eng Part A. 2008 Oct;14(10):1699–707. |
| 18. | ↑ | Tükel HC, Tatli U. Risk factors and clinical outcomes of sinus membrane perforation during lateral window sinus lifting: analysis of 120 patients. → Int J Oral Maxillofac Surg. 2018 Sep;47(9):1189–94. |
| 19. | ↑ | Monsarrat P, Vergnes JN, Planat-Bénard V, Ravaud P, Kémoun P, Sensebé L, Casteilla L. An innovative, comprehensive mapping and multiscale analysis of registered trials for stem cell-based regenerative medicine. → Stem Cells Transl Med. 2016 Jun;5(6):826–35. |





Leave a Reply
Be the First to Comment!