Implant-supported fixed full-arch rehabilitation without bone grafting in severely atrophic maxillae: A 10- to 12-year retro spective follow-up study
December 14, 2018 / Categories: Digital Dentistry, Implant Dentistry
Aizcorbe Vicente, Javier

Peñarrocha Oltra, David

Candel Martí, Eugenia

Camacho Alonso, Fabio

Canullo, Luigi

Peñarrocha Diago, Maria
Abstract
Objective
The objective of this article is to assess the clinical, radiographic and patient-related outcomes of patients with severe atrophy of the maxilla (Cawood and Howell Class V) rehabilitated with fixed full-arch prostheses on dental implants placed in anatomical buttresses and remnant bone.
Materials and methods
An observational retrospective clinical study was performed with a minimum follow-up period of 10 years. An analysis of the following parameters was performed: (a) periimplant parameters (plaque index, modified gingival index, probing pocket depth and keratinized mucosa width); (b) marginal bone loss; (c) implant survival rate; and (d) patient satisfaction based on a visual analog scale (VAS).
Results
Ten patients and 71 dental implants were studied, with a mean follow-up period of 126 months (range: 120–144). The mean plaque index was 1.0 ± 0.5, with a mean probing pocket depth of 2.3 mm (range: 1.0–4.0 mm). Sixty-one percent and 39% of the implants presented a modified gingival index of 1 and 2, respectively, and the mean keratinized mucosa width was 5.8 mm (range: 4.0–10.0 mm). The mean marginal bone loss of the implants was 0.7 ± 0.4 mm (range: 0.0–5.0 mm). The implant survival rate was 97.2%, and the overall mean patient satisfaction score was 90 (range: 0–100). Prosthesis cleaning ease scored lowest on the VAS.
Conclusion
In our limited sample of patients with severe maxillary atrophy (Cawood and Howell Class V), the placement of dental implants in anatomical buttresses and remnant bone, associated with rehabilitation with fixed full-arch prostheses, was found to be an adequate treatment option in the long term regarding implant survival, marginal bone loss, periimplant clinical parameters and patient satisfaction.
Keywords
Dental implants; atrophic maxilla; fixed prosthesis; full arch; long-term; graftless.
Introduction
Tooth loss gives rise to gradual resorption of the alveolar process, with a change in bone and muscle relations and in facial morphology.1Sutton DN, Lewis BR, Patel M, Cawood JI. Changes in facial form relative to progressive atrophy of the edentulous jaws. → Int J Oral Maxillofac Surg. 2004 Oct;33(7):676–82. While most of this resorption occurs in the first year after tooth loss, it continues throughout life and can often give rise to severe bone atrophy both vertically and horizontally.2Rossetti PH, Bonachela WC, Rossetti LM. Relevant anatomic and biomechanical studies for implant possibilities on the atrophic maxilla: critical appraisal and literature review. → J Prosthodont. 2010 Aug;19(6):449–57. Severe bone atrophy of the maxilla (Cawood and Howell Class V) is associated with certain problems, such as reduced perioral tissue support, the impossibility of wearing complete dentures, chewing and speech alterations, and difficulties in placing dental implants owing to the limited amount of available bone.3Cawood JI, Howell RA. A classification of the edentulous jaws. → Int J Oral Maxillofac Surg. 1988 Aug;17(4):232–6.
Many surgical techniques have been proposed for the rehabilitation of this type of patient. These methods can be classified into bone grafting techniques (i.e., guided bone regeneration,4Urban IA, Monje A, Lozada JL, Wang HL. Long-term evaluation of peri-implant bone level after reconstruction of severely atrophic edentulous maxilla via vertical and horizontal guide bone regeneration in combination with sinus augmentation: a case series with 1 to 15 years of loading. → Clin Implant Dent Relat Res. 2017 Feb;19(1):46–55. onlay grafting with autogenous bone blocks,5Sbordone L, Toti P, Menchini-Fabris GB, Sbordone C, Guidetti F. Implant survival in maxillary and mandibular osseous onlay grafts and native bone: a 3-year clinical and computerized tomographic follow-up. → Int J Oral Maxillofac Implants. 2009 Jul–Aug;24(4):695–703.,6Aloy-Prósper A, Peñarrocha-Oltra D, Peñarrocha-Diago MA, Peñarrocha- Diago M. The outcome of intraoral onlay block bone grafts on alveolar ridge augmentations: a systematic review. → Med Oral Patol Oral Cir Bucal. 2015 Mar 1;20(2):e251–8. and inlay autogenous bone grafting7Nyström E, Nilson H, Gunne J, Lundgren S. Reconstruction of the atrophic maxilla with interpositional bone grafting/Le Fort I osteotomy and endosteal implants: a 11–16 year follow-up. → Int J Oral Maxillofac Surg. 2009 Jan;38(1):1–6.), distraction osteogenesis,8Jensen OT, Ringeman JL, Cottam JR, Casap N. Orthognathic and osteoperiosteal flap augmentation strategies for maxillary dental implant reconstruction. → Oral Maxillofac Surg Clin North Am. 2011 May;23(2):301–19. crestal expansion techniques (i.e., split crest9Jensen OT, Cullum DR, Baer D. Marginal bone stability using 3 different flap approaches for alveolar split expansion for dental implants: a 1-year clinical study. → J Oral Maxillofac Surg. 2009 Sep;67(9):1921–30.), the use of special implants (i.e., short dental implants of < 6 mm or narrow dental implants of < 3 mm10Felice P, Soardi E, Pellegrino G, Pistilli R, Marchetti C, Gessaroli M, Esposito M. Treatment of the atrophic edentulous maxilla: short implants versus bone augmentation for placing longer implants. Five-month post-loading results of a pilot randomised controlled trial. → Eur J Oral Implantol. 2011 Autumn;4(3):191–202.) and the modification of the original implant insertion protocol to avoid bone grafting by using areas of residual bone or anatomical buttresses (i.e., zygomatic implants,11Brånemark PI, Gröndhal F, Öhrnell LO, Nilsson P, Petruson B, Svensson B, Engstrand P, Nannmark U. Zygoma fixture in the management of advanced atrophy of the maxilla: technique and long-term results. → Scand J Plast Reconstr Surg Hand Surg. 2004;38(2):70–85.,12Araújo RT, Sverzut AT, Trivellato AE, Sverzut CE. Retrospective analysis of 129 consecutive zygomatic implants used to rehabilitate severely resorbed maxillae in a two-stage protocol. → Int J Oral Maxillofac Implants. 2017 Mar/Apr;32(2):377–84. pterygoid implants,13Candel E, Peñarrocha D, Peñarrocha M. Rehabilitation of the atrophic posterior maxilla with pterygoid implants: a review. → J Oral Implantol. 2012 Sep;38 Spec No:461–6. implant insertion in the maxillary tuberosity,14Lopes LF, Da Silva VF, Santiago JF, Panzarini SR, Pellizer EP. Placement of dental implants in the maxillary tuberosity: a systematic review. → Int J Oral Maxillofac Surg. 2015 Feb;44(2):229–38. tilted implants,15Testori T, Galli F, Fumagalli L, Capelli M, Zuffetti F, Deflorian M, Parenti A, Del Fabbro M. Assessment of long-term survival of immediately loaded tilted implants supporting a maxillary full-arch fixed prosthesis. → Int J Oral Maxillofac Implants. 2017 Jul–Aug;32(4):904–11. palatal implants16Peñarrocha M, Carrillo C, Boronat A, Balaguer J, Peñarrocha MA. Palatal positioning of implants in severely resorbed edentulous maxillae. → Int J Oral Maxillofac Implants. 2009 May–Jun;24(3):527–33.,17Peñarrocha-Oltra D, Candel-Martí E, Peñarrocha-Diago M, Martínez-González JM, Aragoneses JM, Peñarrocha-Diago MA. Palatal positioning of implants in severely atrophic edentulous maxillae: five-year cross-sectional retrospective follow-up study. → Int J Oral Maxillofac Implants. 2013 Jul–Aug;28(4):1140–6. and implants placed in the nasopalatine canal18Peñarrocha D, Candel E, Guirado JL, Canullo L, Peñarrocha M. Implants placed in the nasopalatine canal to rehabilitate severely atrophic maxillae: a retrospective study with long follow-up. → J Oral Implantol. 2014 Dec;40(6):699–706.).
The use of bone grafting to allow implant placement in atrophic maxillae is associated with more frequent complications and higher morbidity, especially when an extraoral donor site is required.19Nkenke E, Neukam FW. Autogenous bone harvesting and grafting in advanced jaw resorption: morbidity, resorption and implant survival. → Eur J Oral Implantol. 2014 Summer;7 Suppl 2:S203–17. The associated increase in financial costs and a longer treatment time can lead, sometimes, to limited patient acceptance of treatment. Additionally, the use of extraoral grafts (i.e., iliac crest) has a nonpredictable resorption pattern, which can be of almost the entire graft, especially in the edentulous maxilla.20Sbordone C, Toti P, Guidetti F, Califano L, Santoro A, Sbordone L. Volume changes of iliac crest autogenous bone grafts after vertical and horizontal alveolar ridge augmentation of atrophic maxillas and mandibles: a 6-year computerized tomographic follow-up. → J Oral Maxillofac Surg. 2012 Nov;70(11):2559–65. The use of short and narrow implants is a promising alternative concept for the treatment of the atrophic maxilla, but the lack of trials for this specific situation with follow-ups of at least 5 years indicate caution regarding results.21Esposito M, Barausse C, Pistilli R, Sammartino G, Grandi G, Felice P. Short implants versus bone augmentation for placing longer implants in atrophic maxillae: one-year post-loading results of a pilot randomised controlled trial. → Eur J Oral Implantol. 2015 Autumn;8(3):257–68.
The use of anatomical buttresses and the residual bone is a predictable way to rehabilitate the atrophic maxilla with dental implants and fixed full-arch prostheses, and several studies detail these techniques.22Alzoubi F, Bedrossian E, Wong A, Farrell D, Park C, Indresano T. Outcomes assessment of treating completely edentulous patients with a fixed implant-supported profile prosthesis utilizing a graftless approach. Part 1: clinically related outcomes. → Int J Oral Maxillofac Implants. 2017 Jul–Aug;32(4):897–903.,23Busenlechner D, Mailath-Pokorny G, Haas R, Fürhauser R, Eder C, Pommer B, Watzek G. Graftless full-arch implant rehabilitation with interantral implants and immediate or delayed loading—part I: reconstruction of the edentulous maxilla. → Int J Oral Maxillofac Implants. 2016 Jul–Aug;31(4):900–5.,24Busenlechner D, Mailath-Pokorny G, Haas R, Fürhauser R, Eder C, Pommer B, Watzek G. Graftless full-arch implant rehabilitation with interantral implants and immediate or delayed loading—part II: transition from the failing maxillary dentition. → Int J Oral Maxillofac Implants. 2016 Sep–Oct;31(5):1150–5.,25Candel-Marti E, Peñarrocha-Oltra D, Bagán L, Peñarrocha-Diago MA, Peñarrocha-Diago M. Palatal positioned implants in severely atrophic maxillae versus conventional implants to support fixed full-arch prostheses: controlled retrospective study with 5 years of follow-up. → Med Oral Patol Oral Cir Bucal. 2015 May 1;20(3):e357–64.,26Fortin Y. Placement of zygomatic implants into the malar prominence of the maxillary bone for apical fixation: a clinical report of 5 to 13 years. → Int J Oral Maxillofac Implants. 2017 May–Jun;32(3):633–41.,27Maló P, Rangert B, Nobre M. All-on-4 immediate-function concept with Brånemark System implants for completely edentulous maxillae: a 1-year retrospective clinical study. → Clin Implant Dent Relat Res. 2005;7 Suppl 1:S88–94.,28Peñarrocha M, Viña JA, Carrillo C, Peñarrocha D, Peñarrocha MA. Rehabilitation of the reabsorbed maxillae with implants in buttresses in patients with combination syndrome. → J Oral Maxillofac Surg. 2012 May;70(5):e322–30. This approach avoids complications and morbidity associated with bone grafting, reduces treatment costs and time, and results in a high patient satisfaction overall.29Candel-Marti E, Peñarrocha-Oltra D, Peñarrocha-Diago MA, Peñarrocha- Diago M. Satisfaction and quality of life with palatal positioned implants in severely atrophic maxillae versus conventional implants supporting fixed full-arch prostheses. → Med Oral Patol Oral Cir Bucal. 2015 Nov 1;20(6):e751–6.,30Alzoubi F, Bedrossian E, Wong A, Farrell D, Park C, Indresano T. Outcome assessment of treating completely edentulous patients with a fixed implant-supported profile prosthesis utilizing a graftless approach. Part 2: patient-related outcomes. → Int J Oral Maxillofac Implants. 2017 Sep–Oct;32(5):1080–5. Nevertheless, these types of techniques are not free of complications and an expert surgeon is required, especially for zygomatic implants.31Araújo RT, Sverzut AT, Trivellato AE, Sverzut CE. Retrospective analysis of 129 consecutive zygomatic implants used to rehabilitate severely resorbed maxillae in a two-stage protocol. → Int J Oral Maxillofac Implants. 2017 Mar/Apr;32(2):377–84.,32Chrcanovic BR, Abreu MH. Survival and complications of zygomatic implants: a systematic review. → Oral Maxillofac Surg. 2013 Jun;17(2):81–93.,33Duarte LR, Filho HN, Francischone CE, Peredo LG, Brånemark PI. The establishment of a protocol for the total rehabilitation of atrophic maxillae employing four zygomatic fixtures in an immediate loading system— a 30-month clinical and radiographic follow-up. → Clin Implant Dent Relat Res. 2007 Dec;9(4):186–96. Because the anatomy of the atrophic maxilla is different for each patient, it is usual in daily practice that only 1 graftless approach is insufficient, and the combined use of different techniques is essential. However, a lack of studies combining different implant approaches in the same patient exists. For this reason, we sought to study the combined use of different techniques to treat the Cawood and Howell Class V atrophic maxilla and their results in the long term.
The aim of this observational retrospective clinical study was to evaluate the implant survival rate, clinical and radiographic outcomes, and patient satisfaction in patients with severe atrophy of the maxilla rehabilitated with dental implants placed in anatomical buttresses and remnant bone and supporting a full-arch fixed prosthesis with a follow-up of at least 10 years.
Materials and methods
An observational, retrospective clinical study was performed in the Oral Surgery Unit of the University of Valencia, Valencia, Spain, from January 2017 to January 2018, involving patients with severe atrophy of the maxilla and subjected to dental implant rehabilitation. A retrospective chart review was performed to select potential candidate patients. The following inclusion criteria were established:
- severe atrophy of the maxilla (Cawood and Howell Class V; the minimum amount of bone for implant placement was 8 mm in height and 3 mm in width, measured at crestal level) treated with dental implants placed in buttresses and in remnant bone;
- rehabilitation with full-arch fixed prosthesis;
- good general health; and
- a minimum follow-up of 10 years after prosthesis delivery.
Before inclusion in the study, the patients received an explanation of the scope and purposes of the study and were asked to sign an informed consent and data confidentiality form.
-

-
Fig. 1A
Occlusal view of the maxilla before surgery.
-
-
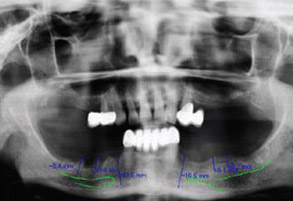
Fig. 1B
Initial panoramic radiograph before surgery.
-

-
Fig. 1C
After flap elevation, 2 pterygoid implants and 4 anterior post-extractive palatal implants were placed.
-
-
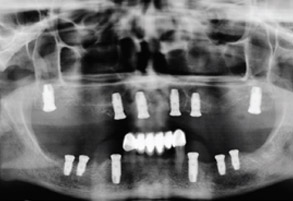
Fig. 1D
Panoramic radiograph after implant placement.
Surgical technique
Before surgery, a panoramic radiograph and a cone beam computed tomography or computed tomography scan was taken of all patients to assess the amount of remaining bone and the presence or absence of maxillary sinus disease. Phibo TSA dental implants with the Avantblast surface (Phibo Dental Solutions) were used. The implants were placed with a combination of drills and osteotomes and were all left submerged (Fig. 1 illustrates a representative clinical case). Sutures were removed 1 week after surgery, and all patients were included in a maintenance program with control visits involving professional prophylaxis every 6 months.
Prosthetic procedure
Healing abutments were connected 3 months after implant placement, and the definitive impressions were obtained 15 days later for preparation of the definitive full-arch screwretained fixed maxillary prosthesis. Implant loading took place 5–6 months after surgery. Fixed hybrid metal–ceramic or fixed hybrid metal–resin prostheses were used for the definitive restoration.
Study variables
Data were collected on patient age and sex, the number of implants and their dimensions, complications, and the date of prosthesis delivery. During the last follow-up visit all the prostheses were removed and the following parameters were recorded:
Clinical parameters:
- plaque index;
- modified gingival index according to the specifications of Mombelli;34Mombelli A, Van Oosten MA, Schürch E, Lang NP. The microbiota associated with successful or failing osseointegrated titanium implants. → Oral Microbiol Immunol. 1987 Dec;2(4):145–51.
- probing pocket depth (measured at 4 points for each implant and the average calculated);
- width of keratinized mucosa in millimeters; and
- the implant survival rate.
-

-
Fig. 1E
Occlusal view of the periimplant soft tissue before definitive prosthesis delivery.
-

-
Fig. 1F
Occlusal view of the fitted screw-retained hybrid metal– resin prosthesis.
Radiographic parameters: Periapical radiographs obtained at prosthesis delivery and after at least 10 years were used to calculate bone loss. Radiographs were obtained with the XMIND intraoral system (Groupe Satelec-Pierre Rolland) and an RVG intraoral digital receptor (Dürr Dental). Periapical radiographs were taken using the paralleling technique with a film holder and an aiming device (Rinn XCP, Dentsply Sirona). If the bone level around the study implants was not clearly visible, a new radio graph was taken. Periimplant marginal bone levels were measured by the same operator, using CliniView software (Version 5.1, Instrumentarium Imaging). Each image was calibrated using the known diameter of the implants. The vertical distance from the outer edge of the implant shoulder (reference point) to the most coronal bone-to-implant contact was measured to the nearest 0.1 mm. From this measurement, we subtracted the measurement of the polished neck of the implant (1.5 mm) to determine exactly the beginning of the treated part. Periimplant marginal bone resorption at the mesial and distal aspect of the implants was calculated from the change in bone level between the baseline (prosthesis delivery) and the last control radiograph available (at least 10-year control); for each pair of measurements, the largest value was used.
Patient-related outcomes: Patient satisfaction was subjectively scored with a visual analog scale (VAS; range: 1–100) used at the time of the study.35Heydecke G, Boudrias P, Awad MA, de Albuquerque RF, Lund JP, Feine JS. Within-subject comparisons of maxillary fixed and removable implant prostheses. → Clin Oral Implants Res. 2003 Feb;14(1):125–30.,36Farzad P, Andersson L, Gunnarsson S, Johansson B. Rehabilitation of severely resorbed maxillae with zygomatic implants: an evaluation of implant stability, tissue conditions, and patients’ opinion before and after treatment. → Int J Oral Maxillofac Implants. 2006 May–Jun;21(3):399–404.,37Pjeturssonn BE, Rast C, Brägger U, Schmidlin K, Zwahlen M, Lang NP. Maxillary sinus floor elevation using the (transalveolar) osteotome technique with or without grafting material. Part I: implant survival and patients’ perception. → Clin Oral Implants Res. 2009 Jul;20(7):667–76. This scale assessed patient satisfaction with the implant-supported prosthesis, measuring the following items: overall satisfaction, comfort and stability, ease of hygiene, ease of speech, esthetics, self-esteem, and function. The patients scored these aspects independently, though a dentist was present in case help or some explanation was needed.
Results
Ten patients with a mean age of 57 years (range: 33–72 years) were included. Of them, 5 were men and 5 women. A total of 71 dental implants were placed in the maxilla (between 6 and 8 implants per patient), with dimensions between 8.5 × 5.5 mm and 16.0 × 4.2 mm. Of these 71 implants, 32 were placed in residual alveolar bone, 3 in the nasopalatine canal, 16 in the pterygomaxillary region, 12 in a palatal position, and 8 simultaneous to a sinus lift procedure, just to obtain bicortical anchorage but without the use of any type of graft (1-stage sinus lift). The mean duration of follow-up was 126 months (range: 120–144 months). At the time of the study, 7 patients had been followed up on for 10 years, 1 patient for 11 years, and 2 for 12 years. None of the patients suffered postoperative complications. Nine patients received hybrid metal–resin prostheses and 1 a hybrid metal–ceramic prosthesis. Regarding prosthesis complications, resin fracture occurred in 2 patients (1 year after loading in 1 case and 4 years after loading in the other), and the problem was solved with simple composite repair (Table 1).
Table 2 shows the main findings of the study. The mean plaque index was 1.0 ± 0.5, with a mean probing pocket depth of 2.3 mm (range: 1.0–4.0 mm). Sixty-one percent and 39% of the implants presented a modified gingival index of 1 and 2, respectively, and the mean keratinized mucosa width was 5.8 mm (range: 4.0–10.0 mm). One nasopalatine implant failed before prosthetic loading, and 1 implant placed in residual alveolar bone failed after loading. The implant survival rate was 97.2%. The mean marginal bone loss was 0.7 ± 0.4 mm (range: 0.0–5.0 mm), with no differences between implant positions. The overall mean patient satisfaction score was 90 (range of the VAS: 0–100). Comfort and stability, function and self-esteem items had the mean highest values (92, 95 and 91, respectively). Prosthesis cleaning ease scored lowest (mean: 72) on the VAS.
-

-
Fig. 1G
Control panoramic radiograph showing correct prosthetic fit.
-

-
Fig. 1H
Occlusal view of the periimplant soft tissue at the 10-year control.
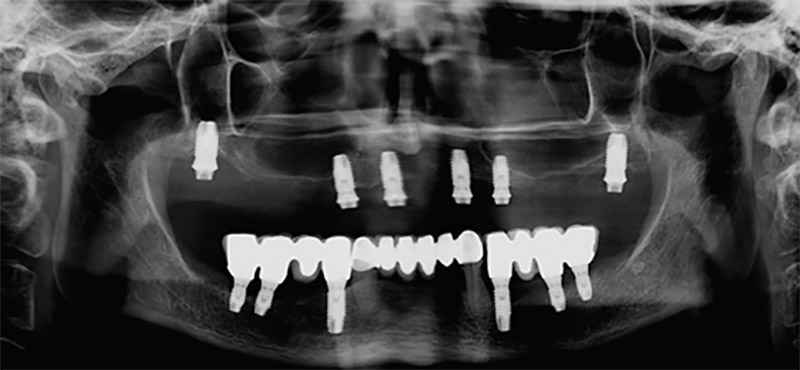
Fig. 1I
Panoramic radiograph at the 10-year control.
Discussion
Severe maxillary atrophy poses problems for conventional implant placement.38Barone A, Orlando B, Tonelli P, Covani U. Survival rate for implants placed in the posterior maxilla with and without sinus augmentation: a comparative cohort study. → J Periodontol. 2011 Feb;82(2):219–26. Bone grafts are an option in such cases, but are not popular among patients, owing to the long treatment times involved, the difficulties and complications related to the surgical procedure and an increase in the treatment cost.39Rosén A, Gynther G. Implant treatment without bone grafting in edentulous severely resorbed maxillas: a long-term follow-up study. → J Oral Maxillofac Surg. 2007 May;65(5):1010–6.
Conventional dental implant placement in remnant bone is an effective alternative for the rehabilitation of these individuals. In this regard, the survival rate for implants in remnant bone is greater than for implants in grafted bone. Widmark et al. reported a survival rate of 87% with conventional implant placement in atrophic maxillae, versus 74% in the case of implants in grafted bone, after a follow-up period of 3–5 years.40Widmark G, Andersson B, Carlsson GE, Lindvall AM, Ivanoff CJ. Rehabilitation of patients with severely resorbed maxillae by means of implants with or without bone grafts: a 3- to 5-year follow-up clinical report. → Int J Oral Maxillofac Implants. 2001 Jan–Feb;16(1):73–9. Rosén and Gynther in turn conducted a study of 19 patients with a mean duration of follow-up of 8–12 years and reported a survival rate of 97%.41Rosén A, Gynther G. Implant treatment without bone grafting in edentulous severely resorbed maxillas: a long-term follow-up study. → J Oral Maxillofac Surg. 2007 May;65(5):1010–6. They concluded that implant placement in the remnant bone of atrophic maxillae is an adequate alternative to bone grafting procedures. In a study by Krekmanov et al. involving 22 patients, the survival rate was found to be 95.7% after a follow-up period of 1–5 years.42Krekmanov L, Kahn M, Rangert B, Lindström H. Tilting of posterior mandibular and maxillary implants for improved prosthesis support. → Int J Oral Maxillofac Implants. 2000 May–Jun;15(3):405–14. More recently, Testori et al. reported a survival rate of 95.1% in a sample of 144 implants placed in atrophic maxillae with a follow- up of 10 years.43Testori T, Galli F, Fumagalli L, Capelli M, Zuffetti F, Deflorian M, Parenti A, Del Fabbro M. Assessment of long-term survival of immediately loaded tilted implants supporting a maxillary full-arch fixed prosthesis. → Int J Oral Maxillofac Implants. 2017 Jul–Aug;32(4):904–11. In our study, the implant survival rate was 97.2% after a mean duration of follow-up of 126 months. Regarding implant position, the survival rate of the implants placed in the nasopalatine canal was especially lower. In the literature, the survival rate of this type of implant was between 84.6% and 100%.44Peñarrocha D, Candel E, Guirado JL, Canullo L, Peñarrocha M. Implants placed in the nasopalatine canal to rehabilitate severely atrophic maxillae: a retrospective study with long follow-up. → J Oral Implantol. 2014 Dec;40(6):699–706.,45De Mello, Faot F, Correa G, Chagas Júnior OL. Success rate and complications associated with dental implants in the incisive canal region: a systematic review. → Int J Oral Maxillofac Surg. 2017 Dec;46(12):1584–91. In our study, the survival rate in this regard was 66.66%. These results can be explained by the limited number of implants (n = 3).
Regarding bone loss, most authors have reported values similar to those of our own series. Aparicio et al. studied 101 conventional implants in 25 patients with atrophic maxillae and recorded a mean bone loss of 1.21 mm after 37 months of follow-up.46Aparicio C, Perales P, Rangert B. Tilted implants as an alternative to maxillary sinus grafting: a clinical, radiologic, and periotest study. → Clin Implant Dent Relat Res. 2001;3(1):39–49. A study by Toljanic et al. recorded a mean bone loss of 0.9 ± 0.8 mm in 46 patients after 1 year of follow-up.47Toljanic JA, Baer RA, Ekstrand K, Thor A. Implant rehabilitation of the atrophic edentulous maxilla including immediate fixed provisional restoration without the use of bone grafting: a review of 1-year outcome data from a long-term prospective clinical trial. → Int J Oral Maxillofac Implants. 2009 May–Jun;24(3):518–26. This figure remained stable from fitting of the prosthesis to 1 year of follow-up. Testori et al. analyzed tilted and axial implants in 41 patients with atrophic maxillae; after a follow-up period of 12 months, they recorded a mean bone loss of 0.9 ± 0.4 mm in axial implants and of 0.8 ± 0.5 mm in tilted implants.48Testori T, Del Fabbro M, Capelli M, Zuffetti F, Francetti L, Weinstein RL. Immediate occlusal loading and tilted implants for the rehabilitation of the atrophic edentulous maxilla: 1-year interim results of a multicenter prospective study. → Clin Oral Implants Res. 2008 Mar;19(3):227–32. In our study, a mean marginal bone loss of 0.7 ± 0.4 mm was observed, in accordance with the literature.
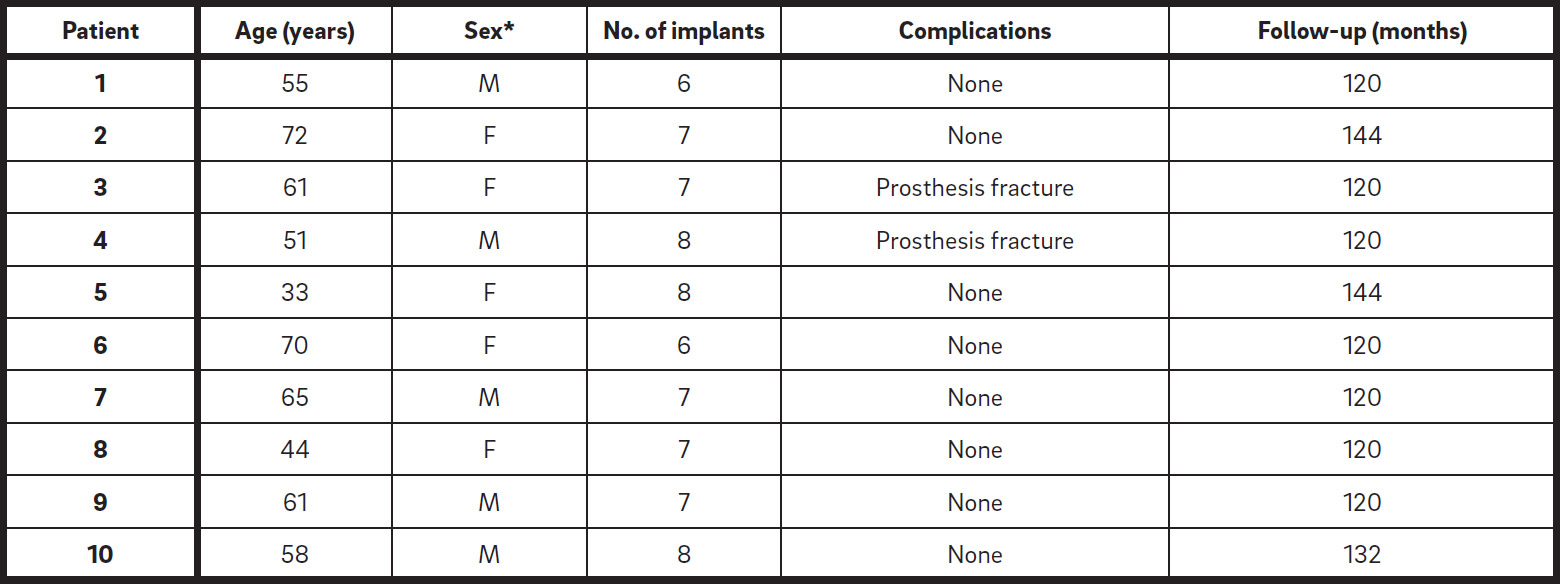
Description of the study sample.
* M = male; F = female.

Results.
PI = plaque index; PPD = probing pocket depth; GI = modified gingival index; KMW = keratinized mucosa width; IS = implant survival; MBL = marginal bone loss; PS = patient satisfaction.
Patient satisfaction was very high, since the procedure proved less invasive and the treatment times were shorter than with other treatment options. In a study by Peñarrocha et al., patients with severe maxillary atrophy rehabilitated with angled and palatine implants showed very high satisfaction scores owing to the reduced time, cost and morbidity associated with the treatment provided.49Peñarrocha MA, Carrillo C, Boronat A, Peñarrocha M. Maximum use of the anterior maxillary buttress in severe maxillary atrophy with tilted, palatally positioned implants: a preliminary study. → Int J Oral Maxillofac Implants. 2010 Jul–Aug;25(4):813–20. Erkarpers et al. likewise recorded very high satisfaction scores in patients with atrophic maxillae rehabilitated with conventional implants and immediate loading.50Erkarpers M, Ekstrand K, Baer RA, Toljanic JA, Thor A. Patient satisfaction following dental implant treatment with immediate loading in the edentulous atrophic maxilla. → Int J Oral Maxillofac Implants. 2011 Mar–Apr;26(2):356–64. The worst result in the present study was obtained for ease of cleaning (72 VAS). In this regard, it is important to ensure that the prosthesis design is easy to clean for patients that usually do not have adequate hygienic skills.
The major limitation of the present observational retrospective clinical study was the small sample of patients (N = 10). It is necessary to carry out studies with larger samples to confirm these results.
Conclusion
In our limited sample of patients with severe maxillary atrophy (Cawood and Howell Class V), the placement of dental implants in anatomical buttresses and remnant bone, rehabilitated with fixed full-arch prostheses, was found to be an adequate treatment option in the long term regarding implant survival, marginal bone loss and periimplant clinical parameters. Patient satis faction was very high; however, it is important to design hygienic (flat or convex) prostheses to facilitate cleaning by the patient at home.
Competing interests
The authors declare that they have no competing interests.
Interview
with Javier Aizcorbe Vicente
Why did you conduct the research reported on in this paper?
For what reasons could others cite your paper?
How could your study’s findings have an impact on dentistry?
What is the relevance of your study’s findings to the daily practice of a dentist?
What are your recommendations for further investigation of the topic of your article?
References
| 1. | ↑ | Sutton DN, Lewis BR, Patel M, Cawood JI. Changes in facial form relative to progressive atrophy of the edentulous jaws. → Int J Oral Maxillofac Surg. 2004 Oct;33(7):676–82. |
| 2. | ↑ | Rossetti PH, Bonachela WC, Rossetti LM. Relevant anatomic and biomechanical studies for implant possibilities on the atrophic maxilla: critical appraisal and literature review. → J Prosthodont. 2010 Aug;19(6):449–57. |
| 3. | ↑ | Cawood JI, Howell RA. A classification of the edentulous jaws. → Int J Oral Maxillofac Surg. 1988 Aug;17(4):232–6. |
| 4. | ↑ | Urban IA, Monje A, Lozada JL, Wang HL. Long-term evaluation of peri-implant bone level after reconstruction of severely atrophic edentulous maxilla via vertical and horizontal guide bone regeneration in combination with sinus augmentation: a case series with 1 to 15 years of loading. → Clin Implant Dent Relat Res. 2017 Feb;19(1):46–55. |
| 5. | ↑ | Sbordone L, Toti P, Menchini-Fabris GB, Sbordone C, Guidetti F. Implant survival in maxillary and mandibular osseous onlay grafts and native bone: a 3-year clinical and computerized tomographic follow-up. → Int J Oral Maxillofac Implants. 2009 Jul–Aug;24(4):695–703. |
| 6. | ↑ | Aloy-Prósper A, Peñarrocha-Oltra D, Peñarrocha-Diago MA, Peñarrocha- Diago M. The outcome of intraoral onlay block bone grafts on alveolar ridge augmentations: a systematic review. → Med Oral Patol Oral Cir Bucal. 2015 Mar 1;20(2):e251–8. |
| 7. | ↑ | Nyström E, Nilson H, Gunne J, Lundgren S. Reconstruction of the atrophic maxilla with interpositional bone grafting/Le Fort I osteotomy and endosteal implants: a 11–16 year follow-up. → Int J Oral Maxillofac Surg. 2009 Jan;38(1):1–6. |
| 8. | ↑ | Jensen OT, Ringeman JL, Cottam JR, Casap N. Orthognathic and osteoperiosteal flap augmentation strategies for maxillary dental implant reconstruction. → Oral Maxillofac Surg Clin North Am. 2011 May;23(2):301–19. |
| 9. | ↑ | Jensen OT, Cullum DR, Baer D. Marginal bone stability using 3 different flap approaches for alveolar split expansion for dental implants: a 1-year clinical study. → J Oral Maxillofac Surg. 2009 Sep;67(9):1921–30. |
| 10. | ↑ | Felice P, Soardi E, Pellegrino G, Pistilli R, Marchetti C, Gessaroli M, Esposito M. Treatment of the atrophic edentulous maxilla: short implants versus bone augmentation for placing longer implants. Five-month post-loading results of a pilot randomised controlled trial. → Eur J Oral Implantol. 2011 Autumn;4(3):191–202. |
| 11. | ↑ | Brånemark PI, Gröndhal F, Öhrnell LO, Nilsson P, Petruson B, Svensson B, Engstrand P, Nannmark U. Zygoma fixture in the management of advanced atrophy of the maxilla: technique and long-term results. → Scand J Plast Reconstr Surg Hand Surg. 2004;38(2):70–85. |
| 12, 31. | ↑ | Araújo RT, Sverzut AT, Trivellato AE, Sverzut CE. Retrospective analysis of 129 consecutive zygomatic implants used to rehabilitate severely resorbed maxillae in a two-stage protocol. → Int J Oral Maxillofac Implants. 2017 Mar/Apr;32(2):377–84. |
| 13. | ↑ | Candel E, Peñarrocha D, Peñarrocha M. Rehabilitation of the atrophic posterior maxilla with pterygoid implants: a review. → J Oral Implantol. 2012 Sep;38 Spec No:461–6. |
| 14. | ↑ | Lopes LF, Da Silva VF, Santiago JF, Panzarini SR, Pellizer EP. Placement of dental implants in the maxillary tuberosity: a systematic review. → Int J Oral Maxillofac Surg. 2015 Feb;44(2):229–38. |
| 15, 43. | ↑ | Testori T, Galli F, Fumagalli L, Capelli M, Zuffetti F, Deflorian M, Parenti A, Del Fabbro M. Assessment of long-term survival of immediately loaded tilted implants supporting a maxillary full-arch fixed prosthesis. → Int J Oral Maxillofac Implants. 2017 Jul–Aug;32(4):904–11. |
| 16. | ↑ | Peñarrocha M, Carrillo C, Boronat A, Balaguer J, Peñarrocha MA. Palatal positioning of implants in severely resorbed edentulous maxillae. → Int J Oral Maxillofac Implants. 2009 May–Jun;24(3):527–33. |
| 17. | ↑ | Peñarrocha-Oltra D, Candel-Martí E, Peñarrocha-Diago M, Martínez-González JM, Aragoneses JM, Peñarrocha-Diago MA. Palatal positioning of implants in severely atrophic edentulous maxillae: five-year cross-sectional retrospective follow-up study. → Int J Oral Maxillofac Implants. 2013 Jul–Aug;28(4):1140–6. |
| 18, 44. | ↑ | Peñarrocha D, Candel E, Guirado JL, Canullo L, Peñarrocha M. Implants placed in the nasopalatine canal to rehabilitate severely atrophic maxillae: a retrospective study with long follow-up. → J Oral Implantol. 2014 Dec;40(6):699–706. |
| 19. | ↑ | Nkenke E, Neukam FW. Autogenous bone harvesting and grafting in advanced jaw resorption: morbidity, resorption and implant survival. → Eur J Oral Implantol. 2014 Summer;7 Suppl 2:S203–17. |
| 20. | ↑ | Sbordone C, Toti P, Guidetti F, Califano L, Santoro A, Sbordone L. Volume changes of iliac crest autogenous bone grafts after vertical and horizontal alveolar ridge augmentation of atrophic maxillas and mandibles: a 6-year computerized tomographic follow-up. → J Oral Maxillofac Surg. 2012 Nov;70(11):2559–65. |
| 21. | ↑ | Esposito M, Barausse C, Pistilli R, Sammartino G, Grandi G, Felice P. Short implants versus bone augmentation for placing longer implants in atrophic maxillae: one-year post-loading results of a pilot randomised controlled trial. → Eur J Oral Implantol. 2015 Autumn;8(3):257–68. |
| 22. | ↑ | Alzoubi F, Bedrossian E, Wong A, Farrell D, Park C, Indresano T. Outcomes assessment of treating completely edentulous patients with a fixed implant-supported profile prosthesis utilizing a graftless approach. Part 1: clinically related outcomes. → Int J Oral Maxillofac Implants. 2017 Jul–Aug;32(4):897–903. |
| 23. | ↑ | Busenlechner D, Mailath-Pokorny G, Haas R, Fürhauser R, Eder C, Pommer B, Watzek G. Graftless full-arch implant rehabilitation with interantral implants and immediate or delayed loading—part I: reconstruction of the edentulous maxilla. → Int J Oral Maxillofac Implants. 2016 Jul–Aug;31(4):900–5. |
| 24. | ↑ | Busenlechner D, Mailath-Pokorny G, Haas R, Fürhauser R, Eder C, Pommer B, Watzek G. Graftless full-arch implant rehabilitation with interantral implants and immediate or delayed loading—part II: transition from the failing maxillary dentition. → Int J Oral Maxillofac Implants. 2016 Sep–Oct;31(5):1150–5. |
| 25. | ↑ | Candel-Marti E, Peñarrocha-Oltra D, Bagán L, Peñarrocha-Diago MA, Peñarrocha-Diago M. Palatal positioned implants in severely atrophic maxillae versus conventional implants to support fixed full-arch prostheses: controlled retrospective study with 5 years of follow-up. → Med Oral Patol Oral Cir Bucal. 2015 May 1;20(3):e357–64. |
| 26. | ↑ | Fortin Y. Placement of zygomatic implants into the malar prominence of the maxillary bone for apical fixation: a clinical report of 5 to 13 years. → Int J Oral Maxillofac Implants. 2017 May–Jun;32(3):633–41. |
| 27. | ↑ | Maló P, Rangert B, Nobre M. All-on-4 immediate-function concept with Brånemark System implants for completely edentulous maxillae: a 1-year retrospective clinical study. → Clin Implant Dent Relat Res. 2005;7 Suppl 1:S88–94. |
| 28. | ↑ | Peñarrocha M, Viña JA, Carrillo C, Peñarrocha D, Peñarrocha MA. Rehabilitation of the reabsorbed maxillae with implants in buttresses in patients with combination syndrome. → J Oral Maxillofac Surg. 2012 May;70(5):e322–30. |
| 29. | ↑ | Candel-Marti E, Peñarrocha-Oltra D, Peñarrocha-Diago MA, Peñarrocha- Diago M. Satisfaction and quality of life with palatal positioned implants in severely atrophic maxillae versus conventional implants supporting fixed full-arch prostheses. → Med Oral Patol Oral Cir Bucal. 2015 Nov 1;20(6):e751–6. |
| 30. | ↑ | Alzoubi F, Bedrossian E, Wong A, Farrell D, Park C, Indresano T. Outcome assessment of treating completely edentulous patients with a fixed implant-supported profile prosthesis utilizing a graftless approach. Part 2: patient-related outcomes. → Int J Oral Maxillofac Implants. 2017 Sep–Oct;32(5):1080–5. |
| 32. | ↑ | Chrcanovic BR, Abreu MH. Survival and complications of zygomatic implants: a systematic review. → Oral Maxillofac Surg. 2013 Jun;17(2):81–93. |
| 33. | ↑ | Duarte LR, Filho HN, Francischone CE, Peredo LG, Brånemark PI. The establishment of a protocol for the total rehabilitation of atrophic maxillae employing four zygomatic fixtures in an immediate loading system— a 30-month clinical and radiographic follow-up. → Clin Implant Dent Relat Res. 2007 Dec;9(4):186–96. |
| 34. | ↑ | Mombelli A, Van Oosten MA, Schürch E, Lang NP. The microbiota associated with successful or failing osseointegrated titanium implants. → Oral Microbiol Immunol. 1987 Dec;2(4):145–51. |
| 35. | ↑ | Heydecke G, Boudrias P, Awad MA, de Albuquerque RF, Lund JP, Feine JS. Within-subject comparisons of maxillary fixed and removable implant prostheses. → Clin Oral Implants Res. 2003 Feb;14(1):125–30. |
| 36. | ↑ | Farzad P, Andersson L, Gunnarsson S, Johansson B. Rehabilitation of severely resorbed maxillae with zygomatic implants: an evaluation of implant stability, tissue conditions, and patients’ opinion before and after treatment. → Int J Oral Maxillofac Implants. 2006 May–Jun;21(3):399–404. |
| 37. | ↑ | Pjeturssonn BE, Rast C, Brägger U, Schmidlin K, Zwahlen M, Lang NP. Maxillary sinus floor elevation using the (transalveolar) osteotome technique with or without grafting material. Part I: implant survival and patients’ perception. → Clin Oral Implants Res. 2009 Jul;20(7):667–76. |
| 38. | ↑ | Barone A, Orlando B, Tonelli P, Covani U. Survival rate for implants placed in the posterior maxilla with and without sinus augmentation: a comparative cohort study. → J Periodontol. 2011 Feb;82(2):219–26. |
| 39, 41. | ↑ | Rosén A, Gynther G. Implant treatment without bone grafting in edentulous severely resorbed maxillas: a long-term follow-up study. → J Oral Maxillofac Surg. 2007 May;65(5):1010–6. |
| 40. | ↑ | Widmark G, Andersson B, Carlsson GE, Lindvall AM, Ivanoff CJ. Rehabilitation of patients with severely resorbed maxillae by means of implants with or without bone grafts: a 3- to 5-year follow-up clinical report. → Int J Oral Maxillofac Implants. 2001 Jan–Feb;16(1):73–9. |
| 42. | ↑ | Krekmanov L, Kahn M, Rangert B, Lindström H. Tilting of posterior mandibular and maxillary implants for improved prosthesis support. → Int J Oral Maxillofac Implants. 2000 May–Jun;15(3):405–14. |
| 45. | ↑ | De Mello, Faot F, Correa G, Chagas Júnior OL. Success rate and complications associated with dental implants in the incisive canal region: a systematic review. → Int J Oral Maxillofac Surg. 2017 Dec;46(12):1584–91. |
| 46. | ↑ | Aparicio C, Perales P, Rangert B. Tilted implants as an alternative to maxillary sinus grafting: a clinical, radiologic, and periotest study. → Clin Implant Dent Relat Res. 2001;3(1):39–49. |
| 47. | ↑ | Toljanic JA, Baer RA, Ekstrand K, Thor A. Implant rehabilitation of the atrophic edentulous maxilla including immediate fixed provisional restoration without the use of bone grafting: a review of 1-year outcome data from a long-term prospective clinical trial. → Int J Oral Maxillofac Implants. 2009 May–Jun;24(3):518–26. |
| 48. | ↑ | Testori T, Del Fabbro M, Capelli M, Zuffetti F, Francetti L, Weinstein RL. Immediate occlusal loading and tilted implants for the rehabilitation of the atrophic edentulous maxilla: 1-year interim results of a multicenter prospective study. → Clin Oral Implants Res. 2008 Mar;19(3):227–32. |
| 49. | ↑ | Peñarrocha MA, Carrillo C, Boronat A, Peñarrocha M. Maximum use of the anterior maxillary buttress in severe maxillary atrophy with tilted, palatally positioned implants: a preliminary study. → Int J Oral Maxillofac Implants. 2010 Jul–Aug;25(4):813–20. |
| 50. | ↑ | Erkarpers M, Ekstrand K, Baer RA, Toljanic JA, Thor A. Patient satisfaction following dental implant treatment with immediate loading in the edentulous atrophic maxilla. → Int J Oral Maxillofac Implants. 2011 Mar–Apr;26(2):356–64. |





Leave a Reply
Be the First to Comment!